1693
Can hepatocellular carcinoma surveillance be performed annually instead of every 6 months in at-risk patients with a negative initial MRI examination?1Diagnostic Radiology, Duke University, Durham, NC, United States
Synopsis
This retrospective study investigated the frequency and timing of development of significant hepatic lesions in patients at risk for HCC undergoing surveillance with an initially negative MRI. Out of 70 patients with an initially negative MRI who had mean follow-up of 36 months (range 12-60 months) by contrast-enhanced CT or MRI, no patients developed positive follow up at 1 year. One patient developed a low-risk LI-RADS 3 lesion at 24 months. It may be reasonable to extend the surveillance interval from six months to 12 months in such patients when the first screening examination is negative.
Background & Aim
Hepatocellular carcinoma (HCC) typically occurs in patients with chronic liver disease, and early detection of small lesions (whether precancerous or small cancers) can improve disease outcomes and reduce mortality[1]. Nearly all major international guidelines recommend imaging surveillance for at-risk patients using ultrasound (US) at six-month intervals[2]. However, the sensitivity of US for detecting small lesions is limited, particularly in obese patients or in patients with severe hepatic steatosis. For these patients, contrast-enhanced liver magnetic resonance imaging (MRI) may be performed instead. Liver MRI performs well for the detection of HCC but is associated with a much higher cost per examination. One potential strategy to mitigate the increased cost of MRI screening is to reduce the frequency with which it is performed. For example, if a patient undergoes a liver MRI that is initially negative or shows only benign findings, perhaps subsequent screening examinations could be performed at one year rather than 6-month intervals. Consequently, the purpose of this study was to investigate the frequency and timing of the development of significant hepatic lesions in at-risk patients with an initially negative screening MRI.Methods
This retrospective study included patients with chronic liver disease with an elevated risk of developing HCC. The Liver Imaging and Reporting Data System (LI-RADS, version 2013) was used for liver MRI technical guidelines and lesion assessments[3]. Clinical MRI reports from patients with chronic liver disease imaged in 2013 were reviewed. Consecutively imaged patients were included who had a negative initial screening MRI (the “index” examination) and who had continued surveillance with multiphasic MRI or computed tomography (CT) every 6-12 months for at least 12 months. MRIs showing either no liver lesions or only LI-RADS 1 lesions were considered negative screening examinations. Patients were excluded if the index MRI showed a focal observation of any category other than LR-1, had a prior history of HCC, or had undergone liver transplantation prior to the first follow-up examination. Demographic data, the presences of cirrhosis, the underlying cause of chronic liver disease, and body mass index was collected for each patient. All available multi-phasic CT and MRI examinations that were compliant with the LI-RADS technical guidelines were included in the follow-up assessment. Follow-up examinations (i.e. subsequent screening examinations) were classified as negative (no liver lesions or only LI-RADS1 lesions) or positive (at least one observation of any category other than LI-RADS 1). Intervals with negative follow-up examinations, first occurrence of a positive follow-up examination, and the ultimate outcome of lesions on positive follow-up examinations were recorded.Result
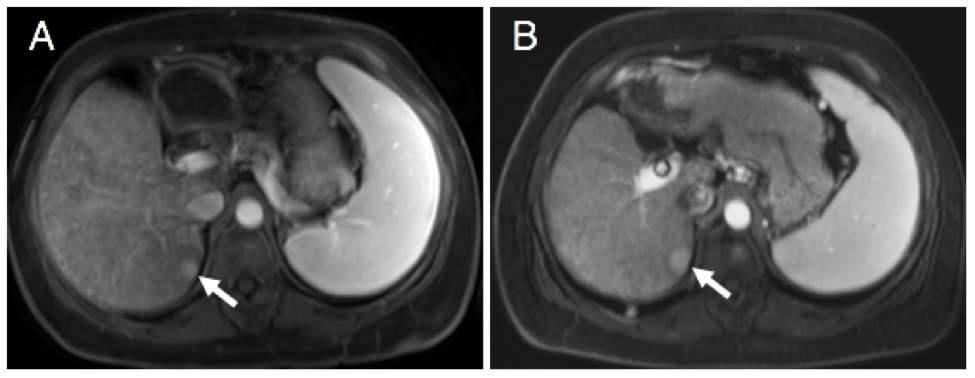
614 patients with chronic liver disease were identified over the study period. 544 patients were excluded for having either a positive index examination, no technically adequate follow-up examination, a prior history of HCC, or liver transplantation prior to one-year follow-up. The remaining 70 patients comprised the study population (45 women, mean age 58 ± 9.5 years). Of these, 65 patients had cirrhosis based on liver biopsy or imaging morphology. Causes of chronic liver disease were non-alcoholic steatohepatitis (n=38), chronic hepatitis C infection (n=9), chronic hepatitis B infection (n=8), and cryptogenic cirrhosis (n=8). In all cases, patients had a technically inadequate prior ultrasound that resulted in a change to surveillance MRI. 67% (47/70) of these patients were obese based on BMI>30 (mean 35 ± 5 kg/m2), and 54% (38/70) had hepatic steatosis by MRI. Mean follow-up duration was 36 ± 14 months (range 12-60 months). Among the 70 patients with negative index screening MRI, none had a positive follow-up examination at either 6 months (n=70) or 12 months (n=70). One patient developed a positive examination during the available follow-up beyond one year. This was a patient with hemochromatosis who had no liver lesions at index MRI and another negative follow-up at one year. On the two year follow-up exam, a 15 mm LI-RADS 3 nodule was identified, coinciding with improvement in background hemosiderosis. This nodule changed minimally over the course of available follow-up for an additional 2 ½ years (17 mm) and did not develop washout or a capsule, remaining a LI-RADS 3 lesion.Conclusion
In patients undergoing MRI rather than US surveillance for HCC, a negative index examination portends a very low rate of development of clinically significant liver nodules at a 1 year follow-up. It may be reasonable to lengthen the screening interval in these patients from six months to 1 year.Acknowledgements
No acknowledgement found.References
1. Fitzmorris, P. and A.K. Singal, Surveillance and Diagnosis of Hepatocellular Carcinoma. Gastroenterology & hepatology, 2015. 11(1): p. 38-46.
2. Tan, C.H., S.-C.A. Low, and C.H. Thng, APASL and AASLD Consensus Guidelines on Imaging Diagnosis of Hepatocellular Carcinoma: A Review %J International Journal of Hepatology. 2011. 2011: p. 11.
3. Kielar, A.Z., et al., LI-RADS version 2018: What is new and what does this mean to my radiology reports? Abdominal Radiology, 2018.
Figures