1691
LI-RADS treatment response criteria for hepatocellular carcinoma after locoregional treatment on contrast-enhanced CT and gadoxetic acid-enhanced MRI: a retrospective validation study using pathologic diagnosis as the reference standard1Department of Radiology, Seoul National University Hospital, Seoul, Korea, Republic of, 2Department of Radiology, Seoul National University College of Medicine, Seoul, Korea, Republic of, 3Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea, Republic of
Synopsis
The liver imaging reporting and data system (LI-RADS) recently introduced a new treatment response algorithm, namely LI-RADS treatment response (LR-TR), for HCCs treated with locoregional therapy. Using pathologic tumor viability as the reference standard, our study showed that LR-TR viable category resulted in sensitivities of 67.3%/74.5% on CT and 75.5%/80.9% on Gd-EOB-MRI; and specificities of 88.6%/88.6% on CT and 80.0%/82.9% on Gd-EOB-MRI, in reviewers 1/2, respectively, which were not significantly different between CT and Gd-EOB-MRI. In addition, our modified TR criteria applying MRI ancillary features demonstrated significantly higher sensitivity (83.6%/88.2%) and comparable specificity (80.0%/77.1%) than LR-TR on CT or MRI.
Introduction
During the follow-up after locoregional therapy (LRT) for hepatocellular carcinoma (HCC), imaging assessment of the presence or absence of viable tumor is critical to determine further management. 1, 2 Recently, the LI-RADS has introduced a per-lesion categorization algorithm on CT or MRI for HCCs treated by LRT, that is, LI-RADS treatment response (LR-TR) 3, 4. It includes categories of viable, equivocal, and nonviable based on dynamic enhancement features. In this study, we retrospectively validated the diagnostic performances of LR-TR on contrast-enhanced CT and gadoxetic acid-enhanced MRI (Gd-EOB-MRI) by using pathologic diagnosis for tumor viability as the reference standard, and also investigated the added value of ancillary features (AFs).Methods
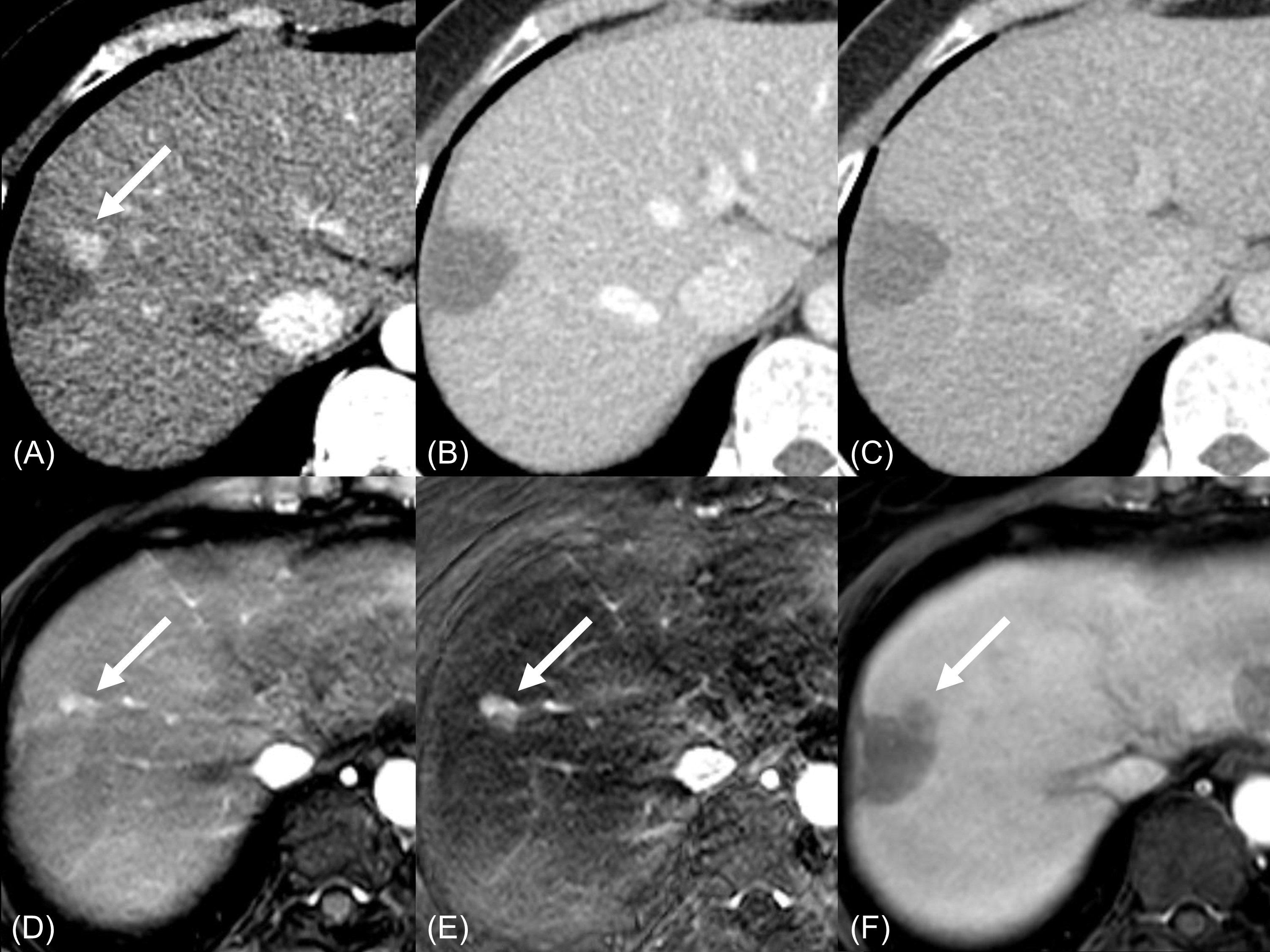
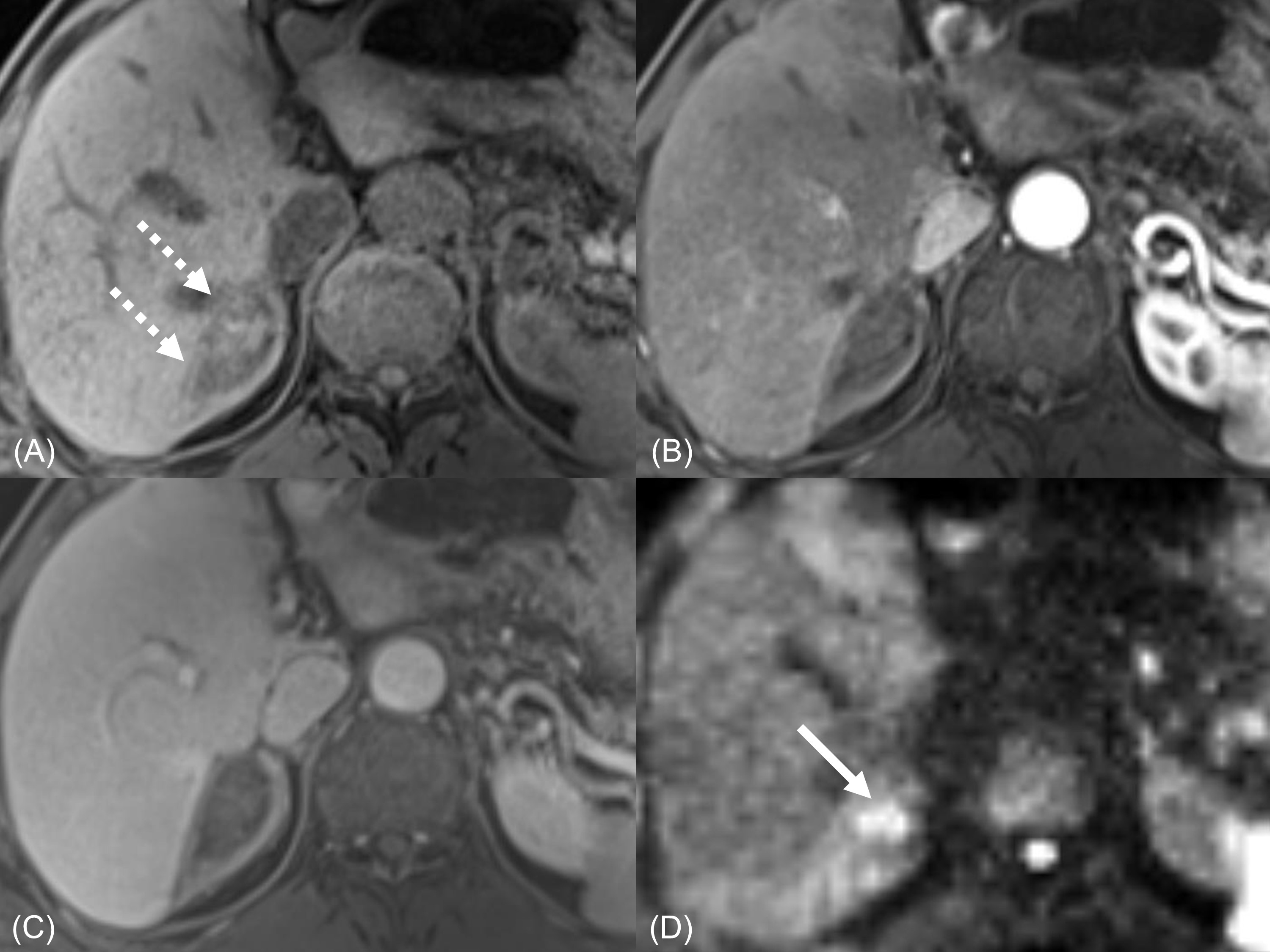
In this retrospective study, we included 145 HCCs which had been previously treated with LRT followed by surgical resection or liver transplantation in 138 patients who had both preoperative four-phase contrast-enhanced CT and Gd-EOB-MRI. On the pathologic reports, complete pathologic necrosis (CPN) (no viable tumor) was confirmed in 35 lesions, and non-CPN (presence of viable tumor) in 110 lesions. For each treated lesion, two independent radiologists were asked to assign TR categories according to i) LR-TR criteria on CT, ii) LR-TR criteria on Gd-EOB-MRI (washout appearance on portal venous phase only), and iii) AF-applied TR criteria on Gd-EOB-MRI (applying imaging features on transitional phase, hepatobiliary phase, diffusion-weighted imaging, and T2-weighted imaging). Using the pathologic tumor viability as the reference standard, the diagnostic performances of TR categories were assessed and compared between criteria using the McNemar test.Results
LR-TR categories according to pathologic tumor viability
Tumors of non-CPN (n=110) were categorized as LR-TR viable/equivocal/nonviable in 67.3% (74/110)/12.7% (14/110)/20.0% (22/110) in reviewer 1 and 74.5% (82/110)/6.4% (7/110)/19.1% (21/110) in reviewer 2 on CT; and 75.5% (83/110)/10.9% (12/110)/13.6% (15/110) in reviewer 1 and 80.9% (89/110)/7.3% (8/110)/11.8% (13/110) in reviewer 2 on Gd-EOB-MRI, respectively. On the other hand, tumors of CPN (n=35) were categorized as LR-TR viable/equivocal/nonviable in 11.4% (4/35)/8.6% (3/35)/80.0% (28/35) and 11.4% (4/35)/5.7% (2/35)/82.9% (29/35) on CT; and 20.0% (7/35)/2.9% (1/35)/ 77.1% (27/35) and 17.1% (6/35)/ 2.9% (1/35)/80.0% (28/35) on Gd-EOB-MRI in reviewers 1 and 2, respectively.
Performance of LR-TR viable category: CT versus Gd-EOB-MRI
LR-TR viable category resulted in sensitivities/specificities of 67.3% (74/110)/88.6% (31/35) and 74.5% (82/110)/88.6% (31/35) on CT, 75.5% (83/110)/80.0% (28/35) and 80.9% (89/110)/82.9% (29/35) on Gd-EOB-MRI, in reviewers 1 and 2, respectively. There were no statistically significant differences in sensitivities; and specificities between CT and Gd-EOB-MRI (Ps>0.05).
Value of ancillary features for the assessment of treatment response on Gd-EOB-MRI
AF-applied TR viable category resulted in sensitivities of 83.6% (92/110) and 88.2% (97/110) in reviewers 1 and 2, respectively, which were significantly higher than LR-TR viable category on CT (67.3% (74/110) and 74.5% (82/110)); or Gd-EOB-MRI (75.5% (83/110) and 80.9% (89/110)), respectively (Ps<0.01). On the contrary, specificities of AF-applied TR criteria (80.0% (28/35) and 77.1% (27/35) in reviewers 1 and 2, respectively) were not significantly different from those of LR-TR on CT or MRI (88.6% (31/35) and 88.6% (31/35), or 80.0% (28/35) and 82.9% (29/35), Ps>0.05). In addition, in comparison to LR-TR on CT or MRI, equivocal category was less frequently assigned in AF-applied TR criteria on MRI (11.7% (17/145), 9.0% (13/145), 0.7% (1/145) in reviewer 1, and 6.2% (9/145), 6.2% (9/145), 1.4% (2/145) in reviewer 2).
Discussion
Our study showed that LR-TR viable category would provide modest sensitivity and specificity for the diagnosis of viable tumor in the treated HCCs by LRT without significant differences between CT and Gd-EOB-MRI. More specifically, approximately 20~30% of non-CPN tumors were false negatively assigned as LR-TR equivocal or non-viable categories; while approximately 10~20% of CPN tumors were false positively assigned as LR-TR viable categories. These results can be explained by the difficulties in detecting small residual or recurred tumors after LRT and in differentiating post-treatment enhancement from viable tumors. Considering that early and accurate diagnosis of viable tumor is essential for the timely and proper management 1, 2, diagnostic performances of LR-TR criteria shown in this study may be not satisfactory. In this regards, our modified TR criteria applying ancillary features on Gd-EOB-MRI may be a good option which can provide higher sensitivity with comparable specificity, and can allow more confident diagnosis with less assignment of equivocal category in comparison to LR-TR criteria.Conclusion
For HCCs treated with LRT, LR-TR categorization may have limited sensitivity for detecting pathologic tumor viability but substantial specificities both on CT and Gd-EOB-MRI. In addition, our modified TR criteria applying ancillary features on Gd-EOB-MRI may help improve sensitivity without significant loss of specificity.Acknowledgements
Institutional Review Board approval was obtained. Written informed consent was waived by the Institutional Review Board.
The authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding.
References
1. Ho M-H, Yu C-Y, Chung K-P, et al. Locoregional therapy-induced tumor necrosis as a predictor of recurrence after liver transplant in patients with hepatocellular carcinoma. Annals of surgical oncology. 2011;18(13):3632-9.
2. Riaz A, Miller FH, Kulik LM, et al. Imaging response in the primary index lesion and clinical outcomes following transarterial locoregional therapy for hepatocellular carcinoma. Jama. 2010;303(11):1062-9.
3. Elsayes KM, Hooker JC, Agrons MM, et al. 2017 version of LI-RADS for CT and MR imaging: An update. RadioGraphics. 2017;37(7):1994-2017.
4. Kielar A, Fowler KJ, Lewis S, et al. Locoregional therapies for hepatocellular carcinoma and the new LI-RADS treatment response algorithm. Abdominal Radiology. 2018;43(1):218-30.
Figures