1690
Features of Preoperative Dynamical Contrast Enhanced 3-T MR Imaging Predicting Early Recurrence for Small (< 3 cm) Hepatocellular Carcinomas after Curative Resection1Department of Radiology, The third affiliated hospital of Sun Yat-sen University, Guangzhou, China, 2Department of Radiology, University of California at San Diego, La Jolla, CA, United States
Synopsis
Small hepatocellular carcinoma (sHCC, < 3 cm) is generally thought to have a good prognosis after surgical resection. However, the prognosis of patients with sHCC is still unsatisfactory because of frequent early recurrence (ER, <1 year) after resection. In our series, 30 % of patients with resected sHCC had ER. Preoperative MR imaging features (corona enhancement and irregular tumor margin) were independent predictors for ER after resection of sHCC.
Introduction
The frequency of detection of small HCC (sHCC, < 3 cm, Guidelines of Japan Cancer Study1) is increasing due to screening of high-risk populations and advances in imaging techniques. However, the treatment of sHCC remains problematic. Liver resection is potentially curative for those patients with well-preserved liver function. However, postoperative ER can be as high as 20-40%2-4. Few studies have attempted to identify MR imaging features for predicting ER after resection of sHCC. Therefore, the purpose of this study was to identify the preoperative predictors (including MR imaging features and tumor markers) for ER after resection of sHCC.Methods
This single-center retrospective study included all patients that between May 2014 to October 2017 had liver dynamic MR imaging one month before curative resection of pathologically proven sHCC with a histologically negative margin and were followed for a minimum of 12 months after surgery or until they died. Pathologically, HCCs were classified as having or not having microvascular invasion (MVI), a validated histologic predictor of ER. ER was defined as a new lesion arising in the remmant liver within 1 year after hepatectomy with the enhancement pattern similar to the previous tumor and meeting LR-5 criteria, and /or as biopsy-comfirmed extrahepatic metastases. All MRI exams were performed on a 3.0T whole-body MRI scanner (Discovery MR750, GE Healthcare, Milwaukee, WI). Two abdominal radiologists (5 and 24 years experience in liver MR imaging) retrospectively reviewed the largest observation in each patient and characterized its LI-RADS v20185 major and ancillary imaging features, as well as some other imaging features. Disagreements were resolved by consensus. Recurrence free survival (RFS) was calculated by the Kaplan-Meier method, and differences in survival between the groups were compared using the log-rank test. A multivariate analysis was used to identify independent predictors and two models (preoperative and postoperative prediction models) were established.Results
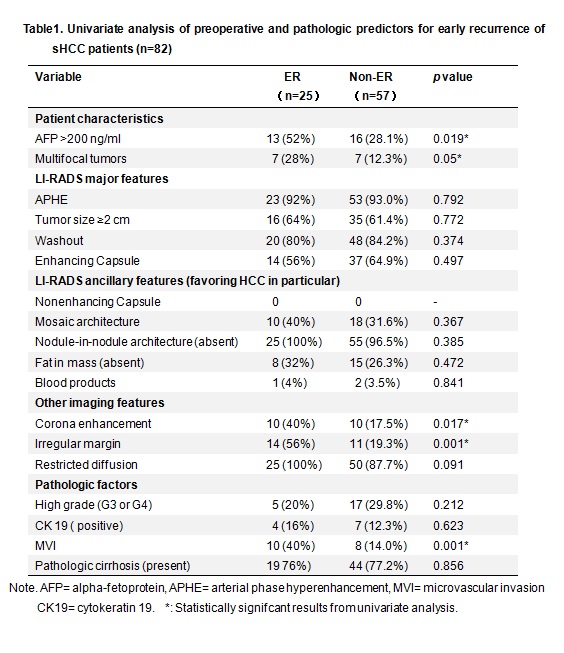
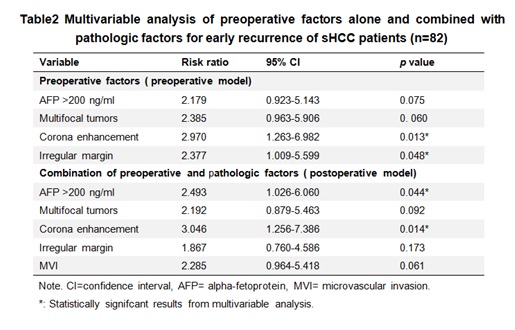
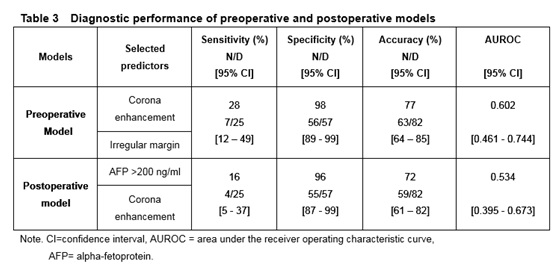
A total of 82 patients with sHCC (assigned as LR-3 [8, 10%], LR-4 [7, 9%], LR-5 [65, 79%], and LR-M [2, 2%]) were included with median follow-up of 24 months. 25 patients (30%) had ER. The mean time to ER was 7.4±2.7 months. The ER rate was higher for HCCs categorized LR-5 or LR-M (31%) than for those categorized LR-3 or LR-4 (27%), but this was not statistically significant (p=0.493). In univariate analyses, preoperative alpha-fetoprotein (AFP) level >200 ng/ml (p=0.019), three MR imaging features (multifocality [p=0.05], corona enhancement [p=0.017], and irregular tumor margin [p=0.001]), and MVI (p=0.001) were associated with ER, Table 1. By multivariate analysis, only corona enhancement and irregular tumor margin were independent predictors in preoperative prediction model, preoperative AFP level >200 ng/ml and corona enhancement (MVI was not) were independent predictors in postoperative prediction model, Table 2. Accuracy, sensitivity, and specificity for ER in preoperative prediction model was 77%, 28%, and 98%, higher than that in postoperative prediction model (72%, 16%, and 96%), Table 3.Discussion
Presence of MVI has been reported to be one of the most important risk factors related to postoperative tumor recurrence2,6. In the current series, two MR imaging features (corona enhancement, irregular tumor margin) were independent predictors for ER in preoperative prediction model, but MVI was not in postoperative prediction model. Our study also demonstrated that preoperative prediction model was slightly superior to postoperative prediction model in predicting ER. Limitations of our study were that it was a retrospective single-center study, and follow up period was relatively short, further study with larger population should be taken to confirm our results.Conclusion
Our results demonstrated preoperative MR imaging features (corona enhancement and irregular tumor margin) have the potential to preoperatively identify high-risk ER patients with sHCC. For these patients, liver transplantation or a wider extent of resection may be considered.Acknowledgements
The authors state that this study has received funding by National Natural Science Foundation of China grant 81271562 (JW) and Science and Technology Program of Guangzhou, China 201704020016 (JW).References
1. Makuuchi M, Kokudo N, Arii S, et al. Development of evidence-based clinical guidelines for the diagnosis and treatment of hepatocellular carcinoma in Japan. Hepatol Res. 2008;38(1):37-51.
2. Yamashita YI, Imai K, Yusa T, et al. Microvascular invasion of single small hepatocellular carcinoma </=3 cm: Predictors and optimal treatments. Ann Gastroenterol Surg. 2018;2(3):197-203.
3. Giuliante F, Ardito F, Pinna AD, et al. Liver resection for hepatocellular carcinoma </=3 cm: results of an Italian multicenter study on 588 patients. J Am Coll Surg. 2012;215(2):244-254.
4. Shah SA, Greig PD, Gallinger S, et al. Factors associated with early recurrence after resection for hepatocellular carcinoma and outcomes. J Am Coll Surg. 2006;202(2):275-283.
5. Chernyak V, Fowler KJ, Kamaya A, et al. Liver Imaging Reporting and Data System (LI-RADS) Version 2018: Imaging of Hepatocellular Carcinoma in At-Risk Patients. Radiology. 2018;181494.
6. Lim KC, Chow PK, Allen JC, et al. Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Ann Surg. 2011;254(1):108-113.
Figures