1688
Prediction for early recurrence of intrahepatic mass-forming cholangiocarcinoma: quantitative MRI combined with prognostic immunohistochemical marker1Diagnostic Radiology, National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and PekingUnion Medical College, Beijing, China, 2MR Research, GE Healthcare, Beijing, China, 3GE Healthcare, Beijing, China
Synopsis
The aim of this study was to develop a nomogram based on pathological characteristics, immunohistochemical molecules, conventional radiological features and texture parameters for predicting the early recurrence (ER) of intrahepatic mass-forming cholangiocarcinoma (IMCC). It was concluded that combining the texture parameters, enhancement pattern and VEGFR could significantly improve the predictive performance of ER.
Purpose
To investigate the predictive performance of combined qualitative and quantitative MRI features before operation and prognostic immunohistochemical marker for early recurrence (ER) of intrahepatic mass-forming cholangiocarcinoma (IMCC).Introduction
Intrahepatic cholangiocarcinoma(ICC) is the second most common primary liver malignancy and is arising in incidence worldwide1. Intrahepatic mass-forming cholangiocarcinoma (IMCC) accounts for a large percentage of ICC. Even after curative resection, the 5-year survival rate is still only 20-35 percent2. The main reason for the poor outcome relates to the incidence of recurrence. Previous studies have revealed several pathological and radiological characteristics associated with postoperative ER of IMCC. Texture analysis (TA) is considered to be an emerging quantitative technique for evaluating entire intra-tumor underlying heterogeneity. Studies in many cancers have shown that TA has the potential for prognosis prediction3.Material and Methods
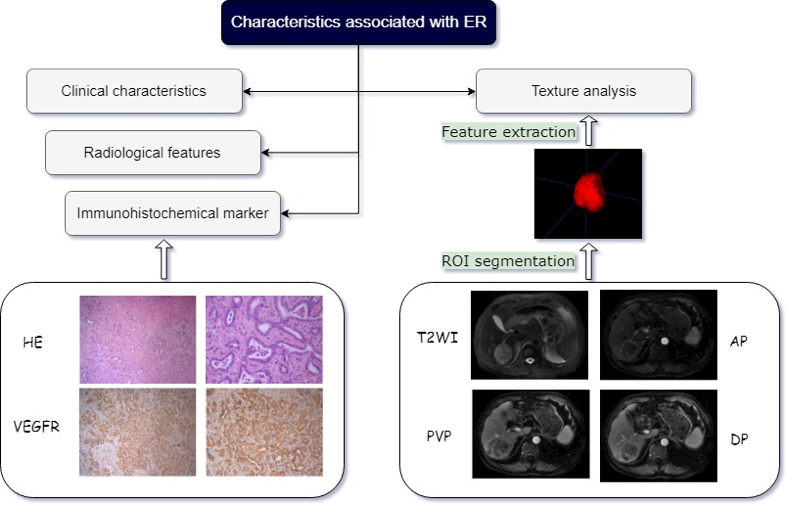
Forty-seven patients with pathologically proven IMCC were enrolled in this retrospective study. Preoperative contrast-enhanced MRI and post-operatively immunohistochemical staining of EGFR, VEGFR, P53 and Ki67 were performed in every patient. The clinicoradiologic and pathological risk factors of ER were identified using univariate analysis. Texture analysis (TA) was performed based on four MR sequences including T2-weighted imaging (T2WI), arterial phase (AP), portal venous phase (PVP) and delayed phase (DP) imaging. The clinicoradiologic-pathological (CRP) model, the TA model, and the combined model were developed, and the receiver operating characteristics curves were used to explore their predictive performance for ER stratification(Fig.1).Results
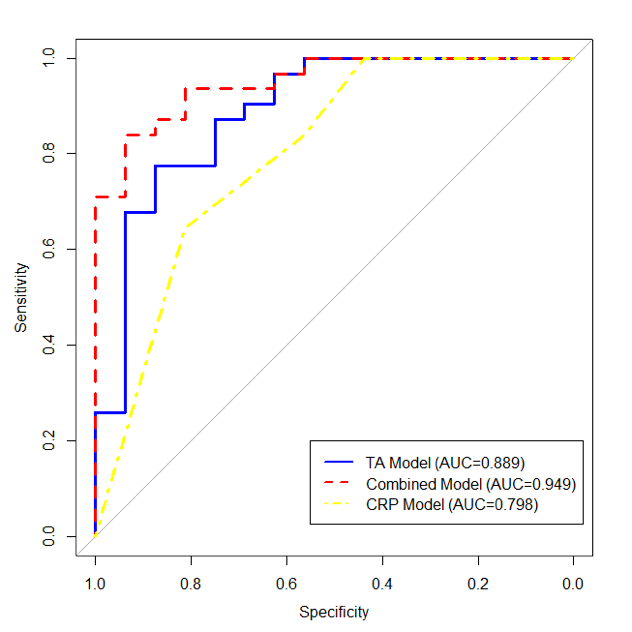
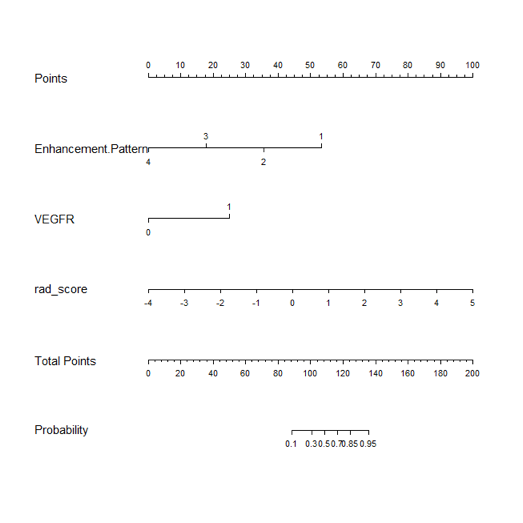
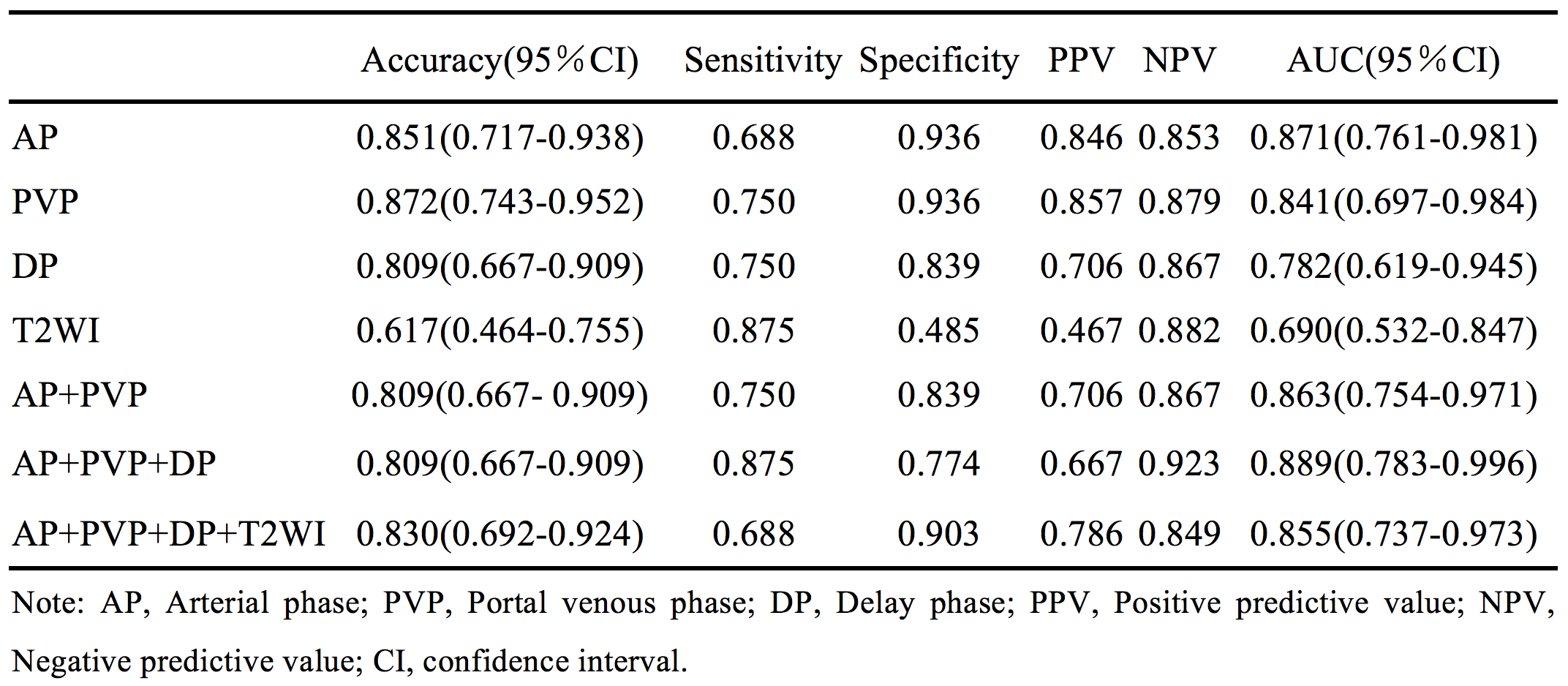
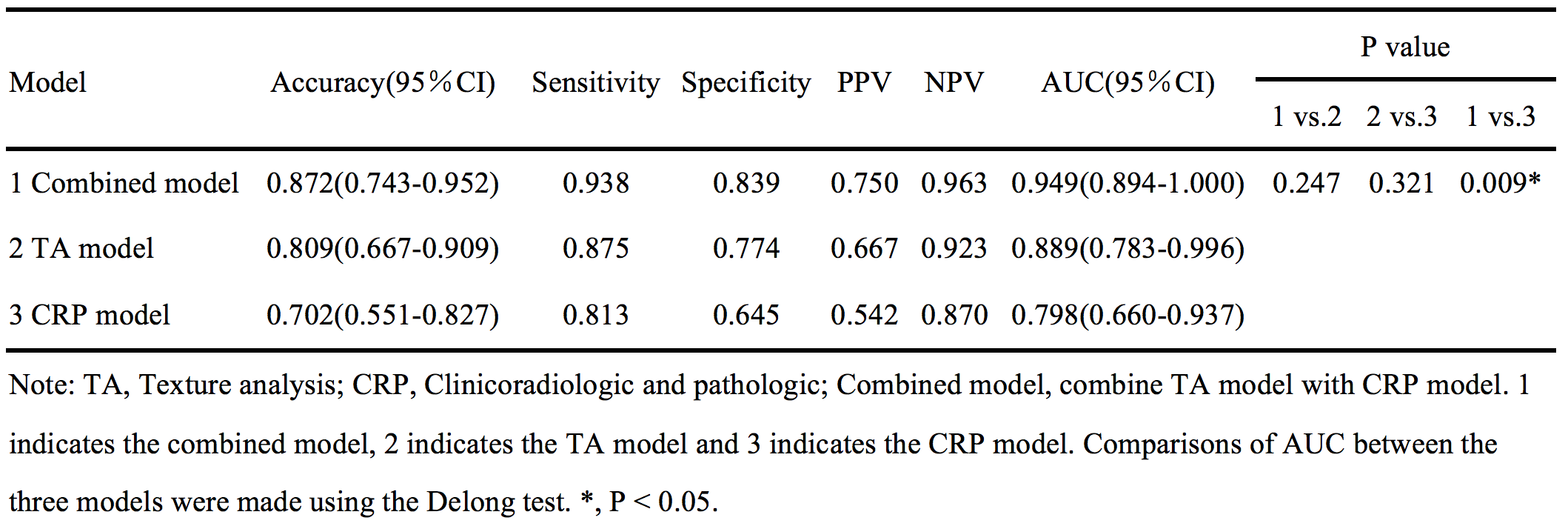
Enhancement pattern and VEGFR showed significant differences between the ER group and non-ER group (P=0.001 and 0.034, respectively). And TA model of AP+PVP+DP (based on AP, PVP, and DP images) presented superior area under curve (AUC) value (0.889, 95% CI:0.783-0.996) among seven TA models, with sensitivity of 0.938 and specificity of 0.839, respectively (Table 1). While the combined model contained enhancement pattern, VEGFR and texture parameters showed preferable predictive performance of ER compared to TA model or CRP model alone, with AUC, sensitivity and specificity of 0.949, 0.875 and 0.774, respectively (Table 2, Fig.2-3).Discussion and Conclusions
Combining the texture parameters, enhancement pattern and VEGFR could significantly improve the AUC, sensitivity, specificity and accuracy for predicting ER compared to TA model or CRP model alone, which indicates that combination of qualitative, quantitative MRI features and immunohistochemical marker maximize the predictive performance of ER. And TA models based on contrast enhanced MR(CE-MR) sequences (AP, PVP, or DP) all showed better specificity and AUC for predicting ER than that of T2WI, which suggested that CE-MR contain more potential tumor heterogeneous information. Furthermore, AP+PVP+DP model showed superior AUC among all the TA models, which was consistent with previous studies4. It demonstrates that multi-phase CE-MR images could provide added value to each other.Acknowledgements
No acknowledgement found.References
1. Razumilava N, Gores GJ. Cholangiocarcinoma. Lancet,2014,383(9935):2168-2179.
2. Spolverato G, Kim Y, Alexandrescu S, et al. Management and Outcomes of Patients with Recurrent Intrahepatic Cholangiocarcinoma Following Previous Curative-Intent Surgical Resection. Ann Surg Oncol,2016,23(1):235-243.
3. Mule S, Thiefin G, Costentin C, et al. Advanced Hepatocellular Carcinoma: Pretreatment Contrast-enhanced CT Texture Parameters as Predictive Biomarkers of Survival in Patients Treated with Sorafenib. Radiology,2018,288(2):445-455.
4. Ueno Y, Forghani B, Forghani R, et al. Endometrial Carcinoma: MR Imaging-based Texture Model for Preoperative Risk Stratification-A Preliminary Analysis. Radiology,2017,284(3):748-757.
Figures