1686
The prediction value of gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid enhanced MRI in Microvascular Invasion of Hepatocellular Carcinoma1Department of Radiology, Third People's Hospital of Nantong,China, Nantong, China
Synopsis
Hepatocellular carcinoma (HCC) is a common malignant tumor in the liver. Microvascular invasion (MVI) is one of the important risk factors affecting the recurrence and prognosis of HCC. Some scholars have predicted MVI through various imaging methods such as CT, MRI and PET, but has not yet reached a unified forecasting standard. Gadoxetate disodium(Gd-EOB-DTPA)is a novel hepatobiliary contrast agent. Peritumoral hypointension in hepatobiliary phase is of great value in predicting MVI, but the related studies are few. In this study, we used multiple parameters to analyze the value of Gd-EOB-DTPA enhanced MRI in predicting MVI qualitatively and quantitatively.
Introduction
Hepatocellular carcinoma (HCC) is a common malignant tumor with a recurrence rate of 40% to 70% after resection for 5 years, however microvascular invasion (MVI) is an important cause affecting postoperative recurrence and prognosis [1-2]. Preoperative prediction of HCC MVI is of great value for prognosis, the choice of comprehensive treatment options and the improvement of tumor-free survival. Gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid (Gd-EOB-DTPA) is a hepatobiliary specific contrast agent and peritumoral hypointension in hepatobiliary phase is important for the prediction of MVI [3]. The purpose of our study is to investigate the predictive value of Gd-EOB-DTPA-enhanced MR in HCC MVI.Methods
Result
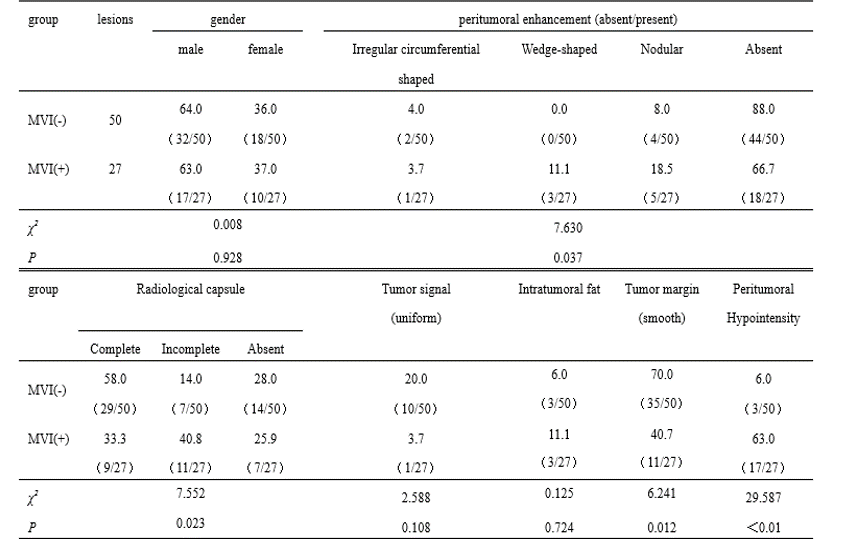
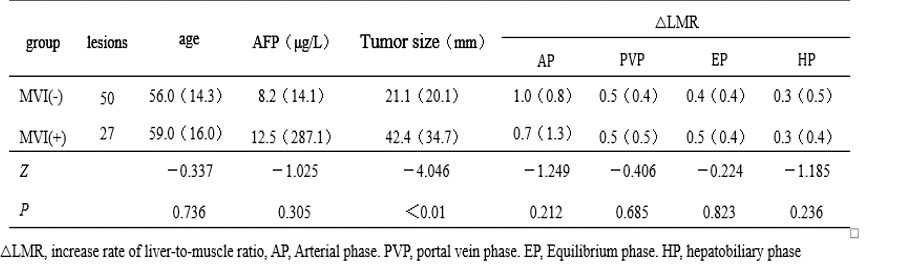
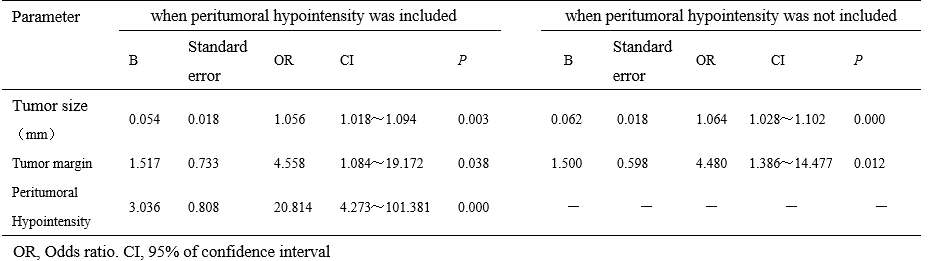
There were 27 lesions in 26 cases of MVI-positive group and 50 lesions in 44 cases of MVI-negative group. There were significant differences between the MVI-negative group and the MVI-positive group in peritumoral enhancement, tumor capsule, tumor margin and peritumoral hypointensity in the hepatobiliary phase (P<0.05), no significant differences in gender distribution, tumor signal uniformity and intratumoral fat(P>0.05)(table1). It was significantly different in diameter between MVI-negative group and MVI-positive group (P<0.05), but not in age, AFP value and △LMR (P>0.05)(table2). Multivariate logistic regression analysis showed that tumor diameter, non-smooth tumor margin and peritumoral hypointensity were independent risk factors of MVI when peritumoral hypointensity was included, the sensitivity and specificity of the combined diagnosis of MVI were 77.8% and 94.0%,on the other hand,when peritumoral hypointensity was not included, tumor diameter and non-smooth tumor margin were independent risk factors of MVI , the sensitivity and specificity of the combined diagnosis of MVI were 59.3%and 92.0%(table3). The the area under the ROC of pre-1 and pre-2 were 0.900 and 0.816, their difference was statistically significant (P<0.05).Discussion
The hepatobiliary phase
of Gd-EOB-DTPA enhanced MRI is important in diagnosis of liver lesions such
as HCC、liver
focal nodular hyperplasia and in the assessment of liver function. Kim [3] study
showed that peritumoral hypointensity in the hepatobiliary phase could predict HCC MVI preoperatively. In our study, multivariate logistic regression analysis showed that tumor diameter, non-smooth tumor margin and peritumoral hypointensity were independent risk factors of MVI when peritumoral hypointensity was included,and the difference between pre-1 and pre-2 was significant (P<0.05). Thus, peritumoral hypointensity in the hepatobiliary phase is useful in predicting HCC MVI.Conclusion
Hepatobiliary phase of Gd-EOB-DTPA enhanced MR is of great value in predicting HCC MVI.
Acknowledgements
No acknowledgement found.References
[1] Imai K, Yamashita YI, Yusa T, et al. Microvascular invasion in small-sized hepatocellular carcinoma: significance for outcomes following hepatectomy and radiofrequency ablation[J]. Anticancer Res, 2018, 38(2): 1053-1060.
[2] Lim KC, Chow PK, Allen JC, et al. Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria[J]. Ann Surg, 2011, 254(1): 108-113.
[3] Kim KA, Kim MJ, Jeon HM, et al. Prediction of microvascular invasion of hepatocellular carcinoma: usefulness of peritumoral hypointensity seen on gadoxetate disodium-enhanced hepatobiliary phase images[J]. J Magn Reson Imaging, 2012, 35(3): 629-634.
Figures

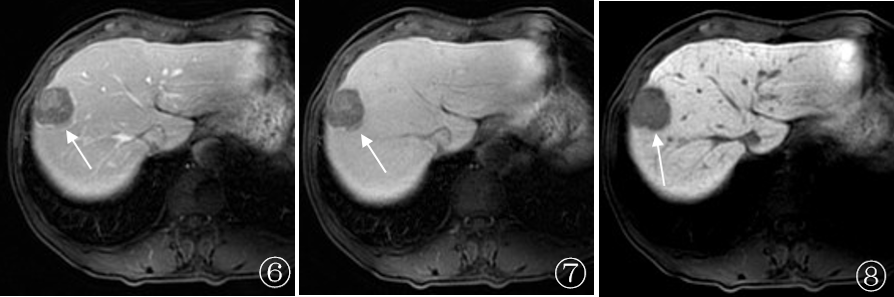
Figure 1~5 Patient, 43 years old, HCC, MVI was confirmed by postoperative pathology. The T2WI axial position (Figure 1) of Gd-EOB-DTPA enhanced MRshowing tumor signal non-uniformity (↑). The arterial phase (Fig. 2) of Gd-EOB-DTPA enhanced MR showing a wedge-shaped enhancement (↑) , during portal phase (Fig. 3) and a transitional phase (Fig. 4) peritumoral enhancement becoming equal signal . The hepatobiliary phase (Fig. 5) of Gd-EOB-DTPA enhanced MR showing peritumor hypointensity (↑)