1685
Quantitative MR image analysis for predicting histopathological growth patterns of liver metastases from colorectal cancer: standard mono-compartmental vs bi-compartmental model1Diagnostic Radiology, McGill University Health Center, Montreal, QC, Canada, 2Epidemiology, Biostatistics and Occupational Health, McGill University Health Center, Montreal, CA, Canada, 3HBP and Transplant Clinical Research, McGill University Health Center, Montreal, QC, Canada, 4Pathology, McGill University Health Center, Montreal, QC, Canada, 5General Surgery, McGill University Health Center, Montreal, QC, Canada
Synopsis
Morphologic and quantitative imagine biomarkers able to reliably and noninvasively determine the different histopathological growth patterns (HGP) of colorectal cancer liver metastases (CRCLM) are currently missing. We aimed to evaluate if a bi-compartmental model (tumour border region, in addition to an inner core region) can outperform the traditional mono-compartmental model for HGP subtype prediction. Our results show an improvement in HGP subtype classification when using the bi-compartmental tumour model, likely because the information arising from the borders are separate from those pertaining to the inner core. As reported, the main differences for HGP tend to occur at the tumour-liver parenchyma interface. This would allow accurate and potentially more effective patient treatment stratification, since the different HGP subtypes have reported variable response rates to anti VEGF-A therapy.
INTRODUCTION
Colorectal cancer liver metastases (CRCLM) have three main histopatological growth patterns (HGP), according to differences at the tumor-liver parenchyma interface: 1) desmoplastic, 2) pushing and 3) replacement. Particularly, the non-desmoplastic patterns mainly show infiltrative features and hepatocytes replacement. They also have a poor prognosis and may not benefit from anti VEGF-A therapy [1, 2, 3, 4]. Currently, there are no definite imaging biomarkers, neither morphologic nor quantitative, which can reliably and noninvasively determine HGP type (desmoplastic vs non-desmoplastic HGP). Typical radiomics image analysis studies in oncology use a mono-compartmental model. A disadvantage with this approach is that spatial localization is lost, as the signal is integrated over the whole tumour region. In the current study we aimed to evaluate if a bi-compartmental model (tumour border region, in addition to an inner core region) can outperform the traditional mono-compartmental model for HGP subtype prediction. This has been based on the reported main differences occurring at the tumor-liver parenchyma interface in HGP at histopathology. Even though both models cover the same spatial area, the bi-compartmental model keeps information pertaining to the tumour border separate from information pertaining to the inner core and does not amalgamate the two. On this basis, the purpose of our study was to assess the ability of quantitative MR image analysis to predict HGP subtypes of CRCLM. Specifically, we modified the traditional radiomics/texture analysis approach to explicitly consider the tumor border.METHODS
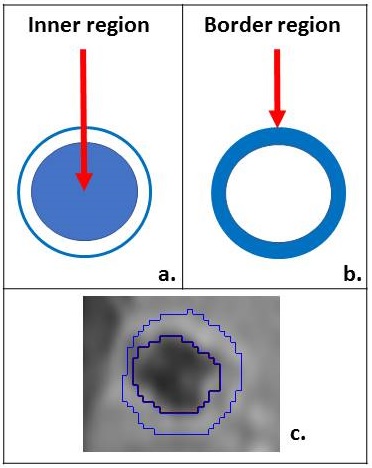
Forty-three patients with proven CRCLM were retrospectively included, with the following criteria: a) liver MRI with contrast (Gadovist, 0.1 ml/kg IV) < 3 months before metastasis resection; b) HGP subtype classification on pathology (desmoplastic/non-desmoplastic). Using in-house software, each lesion was semi-automatically contoured in 3D, into two concentric ROIs on delayed post gadolinium images (acquired 240 second post contrast administration). The lesion’s inner core along borders was delineated as the “inner ROI”; a narrow 3D extension outside the inner core was referred to as the “border ROI”, including adjacent liver parenchyma (Figure 1). The union of these two regions was defined as the “total ROI”. Standard texture analysis (TA) features were extracted from all three ROIs: 6 global histograms (first order) and 22 second-order texture features, at three different levels of image smoothing. Features from the inner and border ROI were combined into one model (bi-compartmental model), while features extracted from the total ROI were used to create a separate model (mono-compartmental model). Each model was used to classify segmented tumors into two groups: desmoplastic or non-desmoplastic, using a random forest classifier. Several classification metrics were assessed for each model, using 1999 non-parametric bootstrap samples.RESULTS
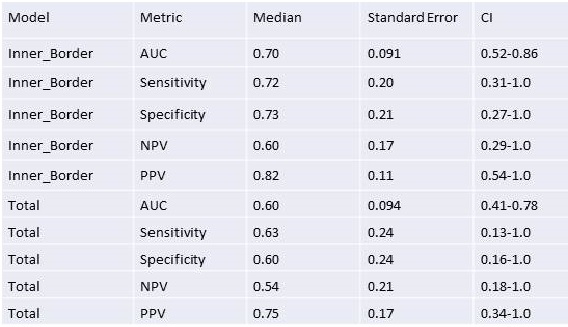
A total of 69 CRCLM were segmented on delayed phase. At histology, 43/69 (62%) were desmoplastic and 26/69 (38%) non-desmoplastic. According to classification metrics for each of the two models under consideration from 1999 non-parametric bootstrap samples (CI 95%), the bi-compartmental model (Inner_Border) demonstrated 0.70 AUC, 0.72 sensitivity, 0.73 specificity, 0.60 NPV, 0.82 PPV. The mono-compartmental model (Total) demonstrated 0.60 AUC, 0.63 sensitivity, 0.60 specificity, 0.54 NPV, 0.75 PPV (Figure 2).DISCUSSION
As reported in the literature, the main differences tend to occur at the tumour-liver parenchyma interface in the different HGP lesions at histopathology. A desmoplastic peripheral rim that separates metastatic cells from normal hepatocytes and promotes peripheral neoangiogenesis is the mainstay of the desmoplastic pattern [1, 2, 3, 4]. Therefore, desmoplastic lesions are likely to better respond to anti VEGF-A therapy. Our results show an improvement in HGP subtype classification when using the bi-compartmental tumour model, as opposed to the mono-compartmental one. This highlights the importance of preserving spatially-localized information within radiomics-type analyses. The improvement in HGP prediction achieved with bi-compartmental tumour model is likely related to the fact that the information arising from the borders are separate from those pertaining to the inner core.CONCLUSION
One of the main challenges in the management of patients with CRCLM is to select patients most likely to respond to anti VEGF-A therapy. Different HGP are reported to have variable response rates to this biologic treatment. A bi-compartmental tumor model from delayed contrast-enhanced MR images can better perform HGP subtype prediction and reflects the underlying tumour histology. This would allow accurate and potentially more effective patient treatment stratification.Acknowledgements
No acknowledgement found.References
1. Frentzas S, Simoneau E, Bridgeman VL, et al. Vessel co-option mediates resistance to anti-angiogenic therapy in liver metastases. Nat Med. 2016;22(11):1294-302.
2. van Dam PJ, van der Stok EP, Teuwen LA, et al. International consensus guidelines for scoring the histopathological growth patterns of liver metastasis. British journal of cancer. 2017;117(10):1427-41.
3. Roviello G, Bachelot T, Hudis CA, et al. The role of bevacizumab in solid tumours: A literature based meta-analysis of randomised trials. Eur J Cancer. 2017;75:245-58.
4. Kim YE, Joo B, Park MS, et al. Dynamic Contrast-Enhanced Magnetic Resonance Imaging as a Surrogate Biomarker for Bevacizumab in Colorectal Cancer Liver Metastasis: A Single-Arm, Exploratory Trial. Cancer Res. 2016;48(4):1210-21.
Figures