1682
T1 mapping on gadoxetic acid-enhanced MR imaging for preoperative prediction of microvascular invasion in hepatocellular carcinoma1Department of Radiology, West China Hospital,Sichuan University, Chengdu, China, 2West China Hospital,Sichuan University, Chengdu, China
Synopsis
Microvascular invasion (MVI) is regarded as one of the independent risk factors for recurrence and poor prognosis of hepatocellular carcinoma (HCC). However, reliable diagnosis of MVI can only be obtained postoperatively. In this study, preoperative T1 mapping on gadoxetic acid-enhanced MR imaging were performed on 79 patients to demonstrate potential imaging biomarkers in prediction of MVI and early recurrence. As a result, pre-contrast T1 relaxation time, reduction rate of T1 relaxation time combined with the presence of peritumoral hypointensity on HBP were found to be potential predictive biomarkers in the preoperative prediction of MVI in HCCs.
Introduction
Microvascular invasion (MVI) is a well-known major prognostic factor of hepatocellular carcinoma (HCC) and one of the predictors of early recurrence within the first year after surgical resection.1 However, the presence of MVI can only be reliably diagnosed by means of histopathologic evaluation.
Gadoxetic acid is a hepatocyte-specific contrast agent and can only be taken up by functioning hepatocytes, which enables the assessment of tumor vascularity as well as other hepatocellular-specific properties within the tumor.2 Several imaging features on gadoxetic acid–enhanced MR imaging, including tumor margin, peritumoral enhancement and peritumoral hypointensity on hepatobiliary phase (HBP) have been found as predictors of MVI and early recurrence.3, 4 However, qualitative assessment of images has the inherent limitation of sensitivity by human visual assessment and varied levels of experience of radiologists.
T1 relaxation measurement on parametric mapping has direct correlation with the concentration of gadoxetic acid, which is likely to be more reliable and accurate compared with qualitative findings or direct signal intensity measurement5 ,therefore, may have the potential ability to preoperatively predict MVI and early recurrence of HCC following hepatic resection.
The aim of our study was to explore the usefulness of T1 mapping on gadexetic acid-enhanced MR imaging in predicting MVI and early recurrence (≤1 year) of HCC after curative resection.
Methods
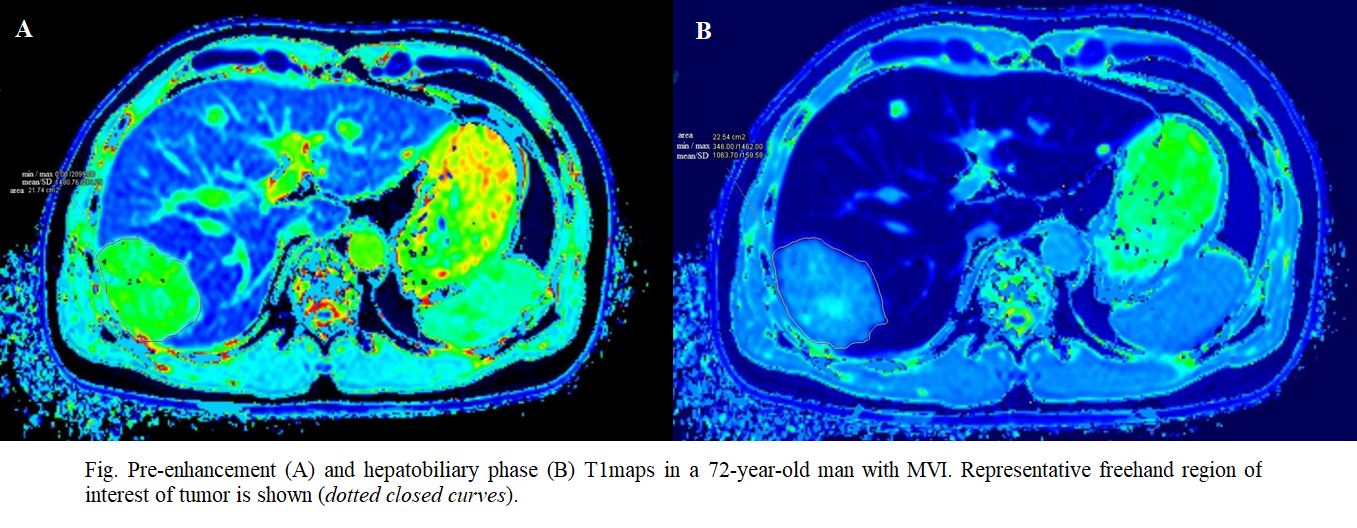
79 patients with surgically confirmed HCC (27 MVI-positive lesions and 52 MVI-negative lesions) were prospectively examined and followed up for at least 1 year after resection. Freehand region of interests (ROIs) were outlined around the largest cross-sectional area of the tumor on pre-enhancement and hepatobiliary phase (HBP)T1 maps. Pre- and postcontrast T1 relaxation time, reduction rate of T1 relaxation time (△%), and radiologic findings (tumor margin, corona enhancement, peritumoral hyperintensity on HBP, and the signal intensity on HBP images) were then assessed. Univariate and multivariate logistic regression analyses were performed to identify the independent predictors of MVI and early recurrence. The diagnostic ability of these parameters was evaluated by receiver operation characteristic (ROC) analysis.Results
27(34%) recurrences were confirmed by imaging follow up. Peritumoral hypointensity on HBP (Odds Ratio [OR]=0.308, 95% confidence interval [CI]: 0.094-1.016; p=0.053), pre-contrast T1 relaxation time (OR=1.048,95%CI: 1.001-1.070; p=0.032) and reduction rate of T1 relaxation time (OR=0.238,95%CI: 0.068-0.814; p=0.005) were identified as independent risk factors for MVI. Reduction rate of T1 relaxation time demonstrated a higher area under the ROC curve (AUC) than pre-contrast T1 relaxation time and peritumoral hypointensity on HBP (AUC=0.702 vs. 0.678 and 0.639, respectively). Combining these independent factors, the AUC of 0.825 (95%CI: 0.727-0.923) was obtained, with sensitivity of 74.1% and specificity of 80.8%, for predicting MVI. For early recurrence, only corona enhancement (p=0.013) and signal intensity on HBP images (p=0.015) were identified as independent predictors.Discussion
In this study, we found that pre-contrast T1 relaxation time and reduction rate of T1 relaxation time on preoperative gadoxetic acid MR imaging had potential ability of predicting MVI of HCCs. Wang et al6 speculated that prolonged T1 relaxation time and reduced reduction rate of T1 relaxation time may be associated with invasion and metastasis of HCC, which could explain that a higher pre-contrast T1 relaxation time and reduction rate of T1 relaxation time in HCCs with the presence of MVI in this study. Meanwhile, peritumoral hypointensity seen on HBP was also identified as a significant predictor of MVI in our study. Lee et al3 have described that peritumoral hypointensity on gadoxetic acid–enhanced HBP images was independently associated with MVI, which was in consistent with our result.
In the present study, corona enhancement and signal intensity on HBP images were found independently associated with early recurrence, which was in accordance with the results of previous studies.7However, one recent study reported that T1 mapping on gadoxetic acid enhanced MRI may be a predictor for early recurrence in HCC,3 while our study showed the conflicting results that no significant correlation was found between T1 values and early recurrence. A possible explanation might be that the early recurrence rate is much lower in our study. The diagnostic ability of T1 mapping in predicting early recurrence after curative resection still required further investigation.
Conclusion
Combing with the presence of peritumoral hypointensity on HBP, T1 mapping on gadoxetic acid enhanced MRI demonstrated an improved discriminative ability in the preoperative prediction of MVI and may guide the clinical-decision making to improve the therapeutic outcome and appropriate patient selection for both liver transplantation and hepatic resection.Acknowledgements
No acknowledgement found.References
1. Lee JI, Lee JW, Kim YS, et al., Analysis of survival in very early hepatocellular carcinoma after resection. J Clin Gastroenterol, 2011. 45(4): p. 366-371.
2. Hamm B, Staks T, Mühler A, et al., Phase I clinical evaluation of Gd-EOB-DTPA as a hepatobiliary MR contrast agent: safety, pharmacokinetics, and MR imaging. Radiology, 1995. 195(3): p. 785-792.
3. Lee S, Kim SH, Lee JE, et al., Preoperative gadoxetic acid-enhanced MRI for predicting microvascular invasion in patients with single hepatocellular carcinoma. J Hepatol, 2017. 67(3): p. 526-534.
4. Hu HT, Shen SL, Wang Z, et al., Peritumoral tissue on preoperative imaging reveals microvascular invasion in hepatocellular carcinoma: a systematic review and meta-analysis. Abdom Radiol (NY), 2018.
5. Haimerl M, Verloh N, Zeman F, et al., Gd-EOB-DTPA-enhanced MRI for evaluation of liver function: Comparison between signal-intensity-based indices and T1 relaxometry. Sci Rep, 2017. 7: p. 43347.
6. Wang WT, Zhu S, Ding Y, et al., T1 mapping on gadoxetic acid-enhanced MR imaging predicts recurrence of hepatocellular carcinoma after hepatectomy. Eur J Radiol, 2018. 103: p. 25-31.
7. An C, Kim DW, Park YN, et al., Single Hepatocellular Carcinoma: Preoperative MR Imaging to Predict Early Recurrence after Curative Resection. Radiology, 2015. 276(2): p. 433-443.
Figures
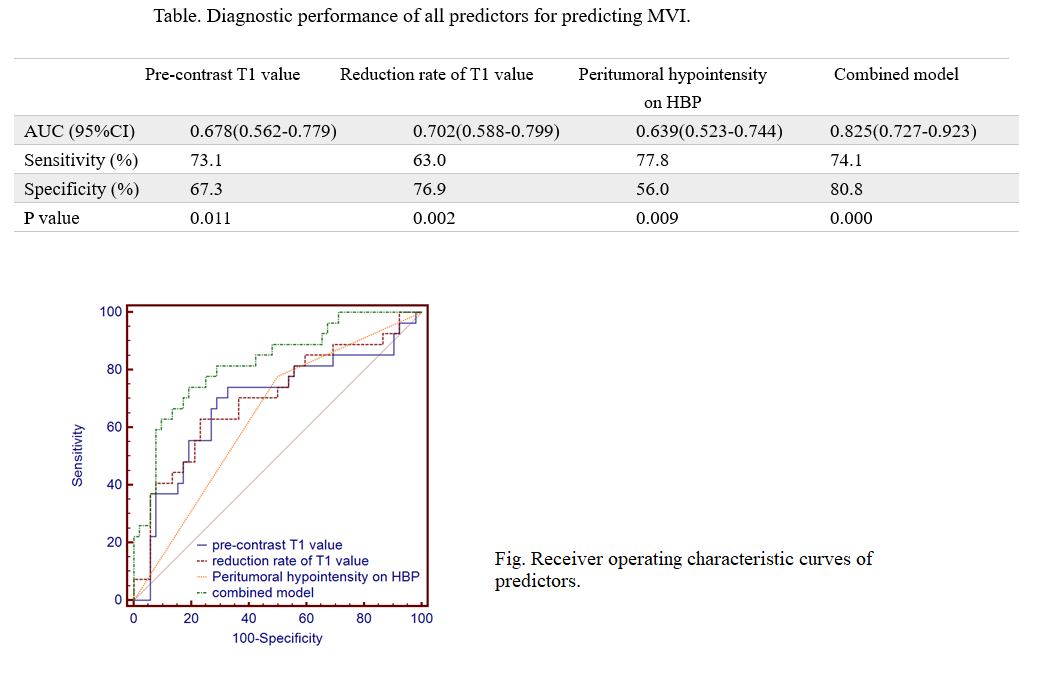
Table. Diagnostic performance of all predictors for predicting MVI
Fig. Receiver operating characteristic curves of predictors for discriminating MVI-positive group from MVI-negative group