1681
Hepatocellular carcinoma: whole-lesion radiomics nomogram on gadoxetic acid-enhanced MR imaging for postoperative early recurrence prediction1Department of Radiology, West China Hospital,Sichuan University, Chengdu, China
Synopsis
The high recurrence rates after curative resection has become a major obstacle for the treatment of HCC. Radiomics has been proposed as a robust and effective imaging analysis method to quantify tumor phenotypic characteristics. In this prospective study, a radiomics model based on preoperative gadoxetic acid-enhanced magnetic resonance (MR) images for preoperative prediction of early recurrence in HCCs was generated, with good discrimination and calibration, and may act as an accurate tool to preoperatively identify high-risk patients and guide clinical decision-making of this population.
Introduction
Hepatocellular carcinoma (HCC) has become the second most common cancer.1 Although hepatic resection is the main curative treatment for HCC with well-preserved liver function, approximately 68%-96% of patients develop postoperative recurrences within 5 years.2,3
Recent studies on magnetic resonance (MR) imaging, particularly with the hepatobiliary contrast agent gadoxetic-acid (Gd-EOB-DTPA), have found several subjective MR findings as non-invasive predictors of early recurrence in HCCs after surgical resection.4, 5 In addition, as a rapidly advancing field of medical image analysis method, radiomics has demonstrated potential in predicting posttreatment survival in the field of oncology.6 Preliminary evidence has indicated that tumor texture features on CT images were potentially predictive of tumor recurrence following curative resection.7 However, few studies have focused on the potential value of radiomics features for early recurrence prediction using gadoxetic-acid MR imaging.
Therefore, the aim of this prospective study was to derive a radiomics nomogram for predicting early recurrence of HCC using clinical characteristics, subjective MR findings and radiomics features on gadoxetic acid-enhanced MRI.
Methods
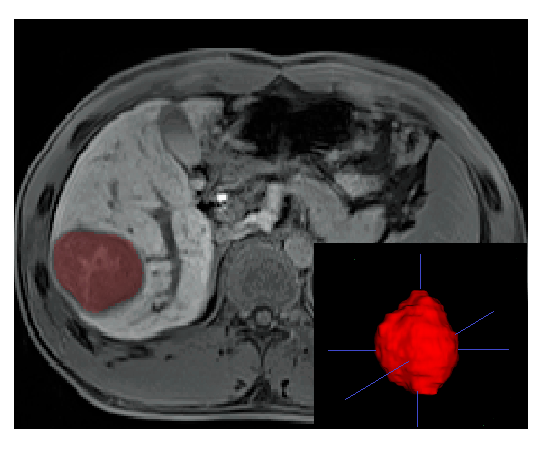
From June 2015 to May 2017, 114 patients (training cohort: n=79; validation cohort: n=35) with surgically confirmed HCC were enrolled in this IRB-approved study. Three-dimensional multi-sequence whole-lesion regions of interest were manually delineated along the tumor margins. Radiomics features were selected to build a radiomics signature using least absolute shrinkage and selection operator (LASSO) method. Clinical risk factors and subjective MR findings were identified and combined to establish a clinic-radiological model. Finally, a radiomics nomogram comprising the radiomics signature and all identified factors was constructed. All models were developed with multivariate logistic regression analysis, and their diagnostic performances and clinical usefulness were measured by receiver operation characteristic (ROC) and decision curves.Results
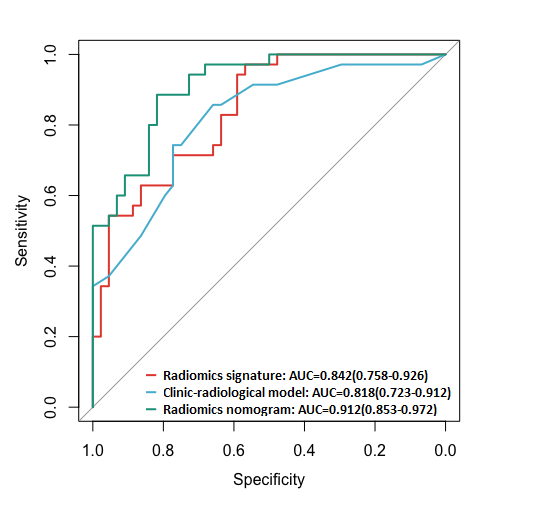
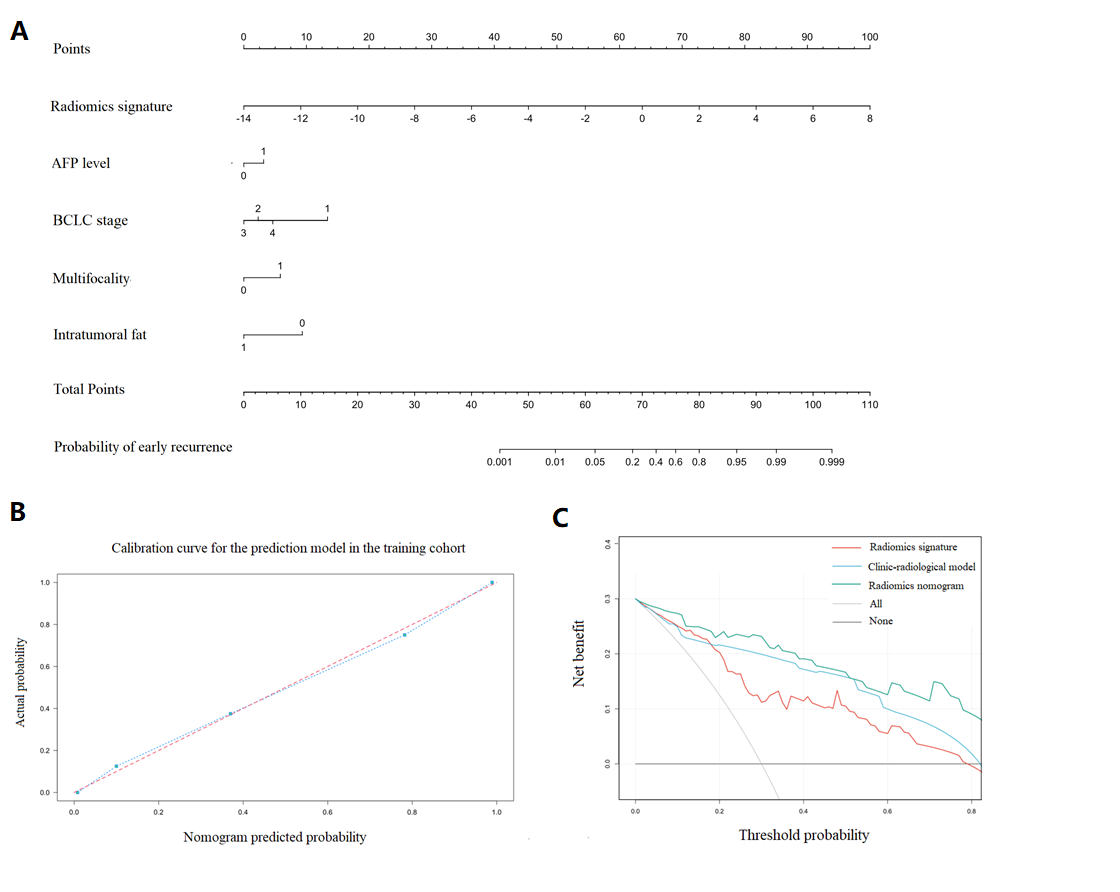
Fifty early recurrences (49.1%) were confirmed by imaging follow-up. The radiomics signature, comprising of 14 selected radiomics features, achieved an area under the ROC curve (AUC) of 0.842 (95% CI, 0.758-0.926) in the training cohort and 0.837 (95% CI, 0.705-0.968) in the validation cohort. Incorporating radiomics signature with alpha-fetoprotein (AFP) level, Barcelona Clinic Liver Cancer (BCLC) stage, multifocality and intratumoral fat, the radiomics nomogram showed excellent discrimination performance in the training (AUC=0.912, 95%CI, 0.853-0.972) and validation cohorts (AUC=0.833, 95%CI, 0.767-0.998) both with incremental clinical usefulness.Discussion
In our study, a multi-sequence MRI-based radiomics model for preoperative prediction of early recurrence in HCCs was generated with good discrimination and calibration.
A few previous results have shown the prognostic value of CT texture features for estimating early recurrence in HCC patients. Zhou et al7 built a radiomics signature based on CT images for preoperative prediction of early recurrence in HCCs, which presented a relatively lower sensitivity of 79.4% and was lack of independent validation. In the present study, the radiomics signature based on MR images demonstrated satisfactory performances in the training and validation cohort (AUC=0.842 and 0.837, respectively), both with markedly high sensitivity (97.1% and 93.3%, respectively), and proved to be an independent predictor for early recurrence in the radiomics nomogram (P=0.008).
High preoperative AFP level, BCLC stage, multifocality and intratumoral fat have been suggested to be effective predictors of early recurrence in previous retrospective studies.8-10 In this study, the proposed radiomics nomogram including these predictors and radiomics signature yielded an improved diagnostic performance in the training cohort (AUC of 0.912 and sensitivity of 88.6%), indicating that the radiomics signature can provide additional prognosis information and has incremental value for conventional approaches; this finding was in consistent with the previous studies.11, 12
However, there are also considerable challenges getting explanation for the correlation between biologic processes and each radiomics signature. Thus, further exploration of radiogeomics study is required to establish a more comprehensive radiogenomics model.
Conclusion
The proposed MR multi-sequence whole-lesion based radiomics nomogram hold great promise in the preoperative prediction of early recurrence for HCC and may serve as an accurate tool to guide clinical treatment decision-making.Acknowledgements
No acknowledgement found.References
1. Torre LA, Bray F, Siegel RL, et al., Global cancer statistics, 2012. CA Cancer J Clin, 2015.
2. Lau WY and Lai EC, Hepatocellular carcinoma: current management and recent advances. Hepatobiliary Pancreat Dis Int, 2008.
3. Poon RT, Fan ST, Lo CM, et al., Long-term survival and pattern of recurrence after resection of small hepatocellular carcinoma in patients with preserved liver function: implications for a strategy of salvage transplantation. Ann Surg, 2002.
4. Lee JI, Lee JW, Kim YS, et al., Analysis of survival in very early hepatocellular carcinoma after resection. J Clin Gastroenterol, 2011.
5. An C, Kim DW, Park YN, et al., Single Hepatocellular Carcinoma: Preoperative MR Imaging to Predict Early Recurrence after Curative Resection. Radiology, 2015. 276(2): p. 433-443.
6. Keek SA, Leijenaar RT, Jochems A, et al., A review on radiomics and the future of theranostics for patient selection in precision medicine. Br J Radiol, 2018: p. 20170926.
7. Zhou Y, He L, Huang Y, et al., CT-based radiomics signature: a potential biomarker for preoperative prediction of early recurrence in hepatocellular carcinoma. Abdom Radiol (NY), 2017. 42(6): p. 1695-1704.
8. Du Z-G, Wei Y-G, Chen K-F, et al., Risk factors associated with early and late recurrence after curative resection of hepatocellular carcinoma: a single institution's experience with 398 consecutive patients. Hepatobiliary & Pancreatic Diseases International, 2014. 13(2): p. 153-161.
9. Wang Z-X, Jiang C-P, Cao Y, et al., Preoperative serum liver enzyme markers for predicting early recurrence after curative resection of hepatocellular carcinoma. Hepatobiliary & Pancreatic Diseases International, 2015. 14(2): p. 178-185.
10. Siripongsakun S, Lee JK, Raman SS, et al., MRI detection of intratumoral fat in hepatocellular carcinoma: potential biomarker for a more favorable prognosis. AJR Am J Roentgenol, 2012. 199(5): p. 1018-1025.
11. Huang Y, Liu Z, He L, et al., Radiomics Signature: A Potential Biomarker for the Prediction of Disease-Free Survival in Early-Stage (I or II) Non-Small Cell Lung Cancer. Radiology, 2016. 281(3): p. 947-957.
12. Meng Y, Zhang Y, Dong D, et al., Novel radiomic signature as a prognostic biomarker for locally advanced rectal cancer. J Magn Reson Imaging, 2018.
Figures