1677
Radiomics features of gastrointestinal stromal tumors (GISTs) based on whole-tumor analysis: the robust imaging biomarkers to stratification and monitoring purpose1Radiology, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, wuhan, China
Synopsis
The diagnosis and
treatment plans of GISTs are relied on pathological confirmation, yet the
biopsy for unresectable GISTs cannot always provide comprehensive information,
which will have an impact on the treatment plan and duration. Radiomics
features based on whole tumor analysis have been confirmed as a robust imaging
biomarkers with good repeatability in some solid tumors. The present study
using the method described above to analyze a group of patients with
pathological confirmed GISTs, to determine which radiomics features are useful
for stratification and monitoring purpose.
purpose
To investigate radiomics features of a group of patients with pathological confirmed GISTs, using volumetric apparent diffusion coefficient (ADC) histogram analysisIntroduction
GISTs are the most common mesenchymal tumors whose biological behavior ranges from benign to malignant1. Accurate preoperative diagnosis and risk stratification of GISTs are very important as it correlates closely with tumor recurrence and prognosis and selection for adjuvant imatinib treatment and treatment duration2. The Choi criteria, only measuring density of a region of interest on a single slice, is recommended to evaluate the efficacy of adjuvant therapy for GIST patients3. Nevertheless, some studies proved that volumetric analysis on solid tumors could avoid selection bias4. Recent studies elucidate the value of diffusion-weighted imaging (DWI) for detection and characterization of GISTs and for early evaluation of tumor response to therapies2,5,6. These studies analyzed the ADC values measured in a single slice of the tumor and they draw ROIs with areas of cystic degeneration and necrosis excluded. The present study is trying to capture the whole tissue information by whole-tumor quantitative ADC histogram analysis, and apply the volumetric ADC to discriminate different risk grade of GISTs with pathological correlationMethods
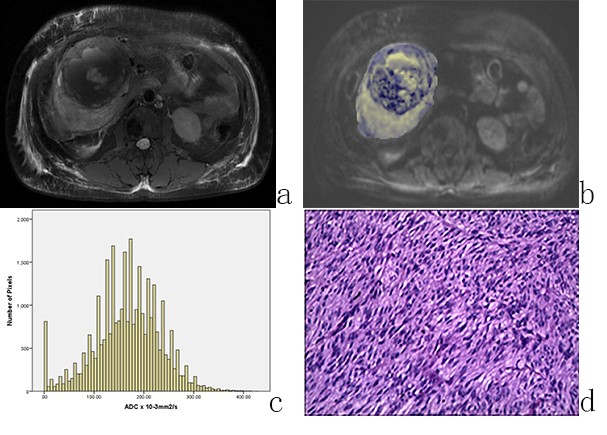
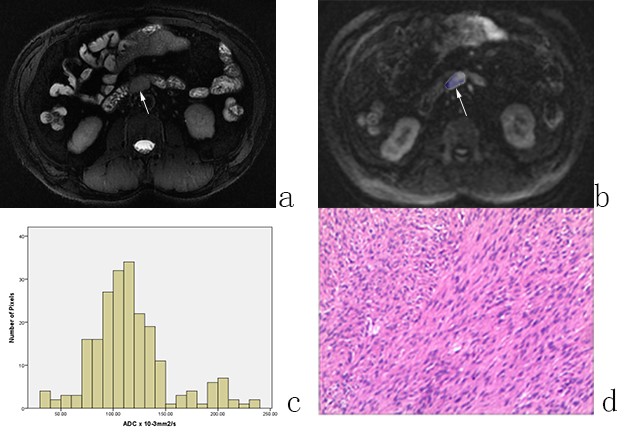
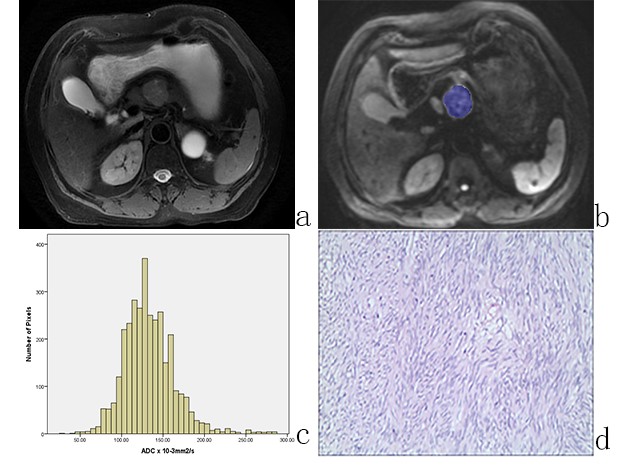
In present study, 24 pathologically confirmed primary GIST patients (11 men, 13 women, median age, 53 years, age range, 29-74 years) with routine abdominal/bowel MRI and DWI (b=0, 800s/mm2) performed at 3 T before surgery were enrolled. The mean interval of MRI and surgery was 8.65 days (range 1-19 days). The whole tumor measurements were performed by one radiologist twice with open source software (Firevoxel; https://files.nyu.edu/hr18/public/projects.html ) on all slices of the lesion and any cystic, necrotic or hemorrhagic were included. Histogram parameters, including the mean ADC value, the median ADC value, ADCmin, ADCmax, ADCStDev, ADC5%, ADC10%, ADC25%, ADC50%, ADC75%, ADC90%, ADC95%, entropy, skewness and kurtosis were obtained.Results
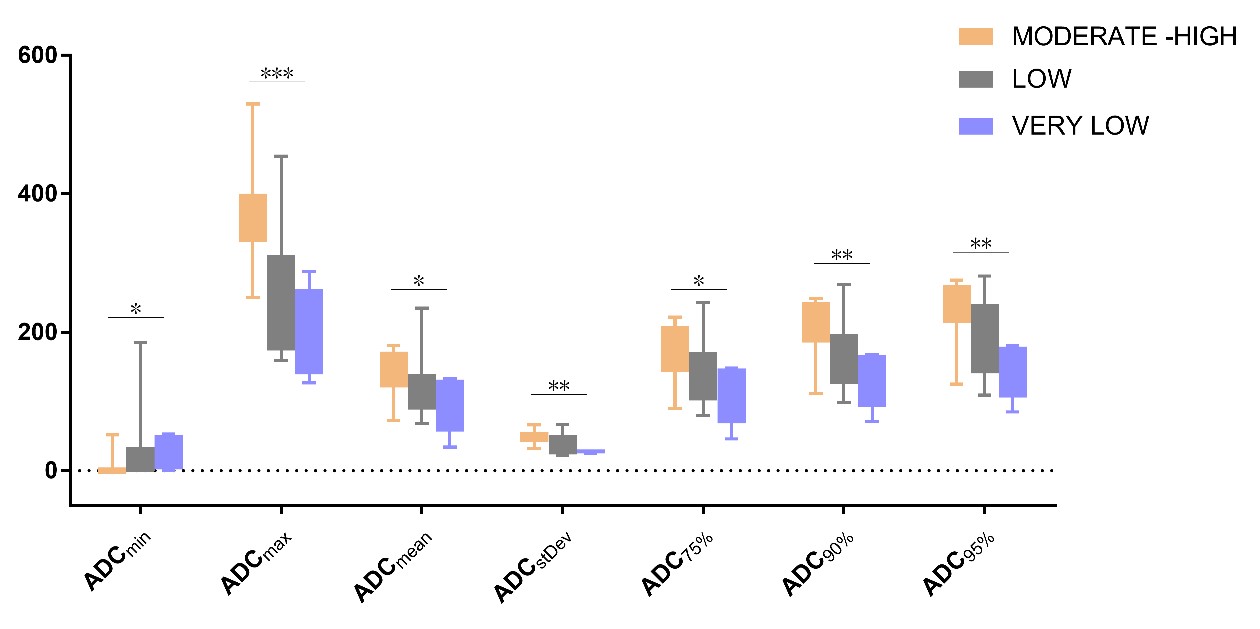
Based on the modified National Institutes of Health (NIH) consensus criteria, there are 8 cases with high risk, 2 cases with intermediate risk, 10 cases with low risk and 4 cases with very low risk. As there are only 2 GISTs with moderate risk, we incorporate the results of it into high-risk group. As the risk grade of GISTs grows, the value of ADCmean, ADCmax, ADCStDev, ADC75%, ADC90% and ADC95% increased and ADCmin correlates negatively with the risk grade (Fig.1).Discussion
The present study shows that ADC histogram parameters including ADCmin, ADCmean, ADCmax, ADCStDev, ADC75%, ADC90% and ADC95% are helpful in risk stratification of GISTs. The trend of results is opposite to the previous study except for ADCmin. This may be attributed to the whole-tumor analysis method contains information of all voxels including necrosis and cystic degeneration. This may become a more effective method in depicting characters of ADC value of GISTs, which can be used not only for preoperative grading diagnosis of primary resectable tumors, but also for unresectable grading diagnosis that requires characterization to identify further therapeutic agents and drug selection and treatment duration selection, in addition to serve as baseline value for efficacy assess of the response of GISTs to molecular targeted agents7,8Conclusion
ADC histogram analysis based on the whole volume of the tumor can provide useful diagnosis information in differentiating risk grade of GISTs.Acknowledgements
We thank Jingyu Lu, Hao Yu for their important contributions to this studyReferences
1. Joensuu H, Hohenberger P, Corless CL. Gastrointestinal stromal tumour. Lancet 2013; 382(9896): 973-83.
2. Kang TW, Kim SH, Jang KM, et al. Gastrointestinal stromal tumours: correlation of modified NIH risk stratification with diffusion-weighted MR imaging as an imaging biomarker. Eur J Radiol 2015; 84(1): 33-40.
3. Choi H, Charnsangavej C, Faria SC, et al. Correlation of computed tomography and positron emission tomography in patients with metastatic gastrointestinal stromal tumor treated at a single institution with imatinib mesylate: proposal of new computed tomography response criteria. J Clin Oncol 2007; 25(13): 1753-9.
4. Li Z, Bonekamp S, Halappa VG, et al. Islet Cell Liver Metastases: Assessment of Volumetric Early Response with Functional MR Imaging after Transarterial Chemoembolization. Radiology 2012; 264(1): 97-109.
5. Zhou HY, Zhang XM, Zeng NL, Jian SH, Tang W. Use of conventional MR imaging and diffusion-weighted imaging for evaluating the risk grade of gastrointestinal stromal tumors. J Magn Reson Imaging 2012; 36(6): 1395-401.
6. Tang L, Zhang XP, Sun YS, et al. Gastrointestinal stromal tumors treated with imatinib mesylate: Apparent diffusion coefficient in the evaluation of therapy response in patients. Radiology 2011; 258(3): 729-38.
7. Gong NJ, Wong CS, Chu YC, Gu J. Treatment response monitoring in patients with gastrointestinal stromal tumor using diffusion-weighted imaging: preliminary results in comparison with positron emission tomography/computed tomography. Nmr Biomed 2013; 26(2): 185-92.
8. Wong CS, Gong N, Chu YC, et al. Correlation of measurements from diffusion weighted MR imaging and FDG PET/CT in GIST patients: ADC versus SUV. Eur J Radiol 2012; 81(9): 2122-6.
Figures