1676
Pre and Postprandial Hemodynamics of the Gastroduodenal Artery in Patients Suspected of Chronic Mesenteric Ischemia using 4D Flow MRI1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Chronic mesenteric ischemia (CMI) causes reduced intestinal blood flow, often from mesenteric occlusions. However, collaterals exist and help compensate for reduced blood flow. This study utilizes 4D flow MRI to quantify hemodynamics in the gastroduodenal artery (GDA), a collateral between the celiac and superior mesenteric arteries, in controls (N=14) and patients suspected of CMI (N=14) before and after a meal. There was no significant difference in preprandial, postprandial, or percent flow change values between groups. However, pathology-dependent flow patterns were evident within the ischemia group. Follow-up studies with larger cohorts are warranted to further examine this finding.
Introduction
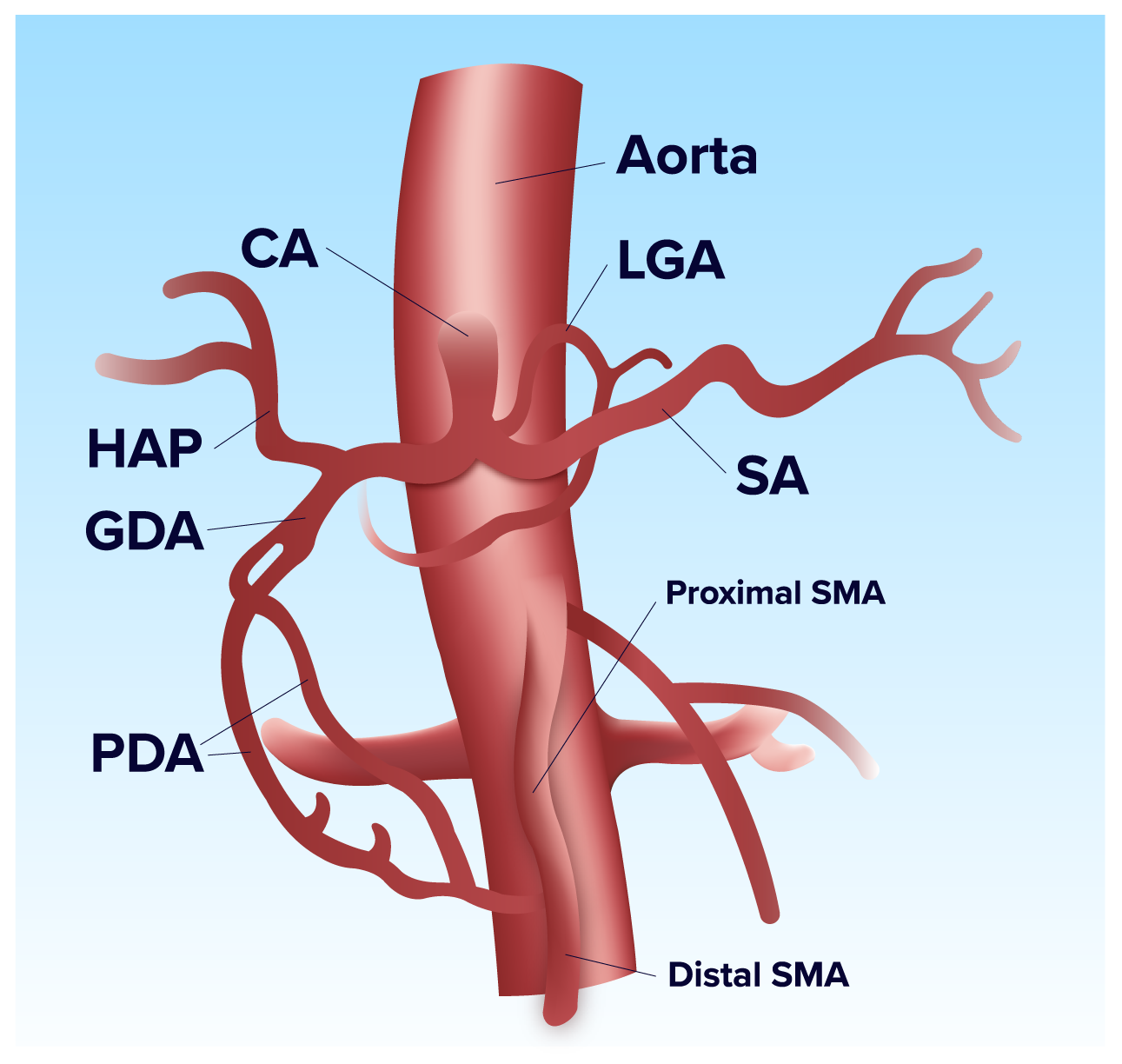
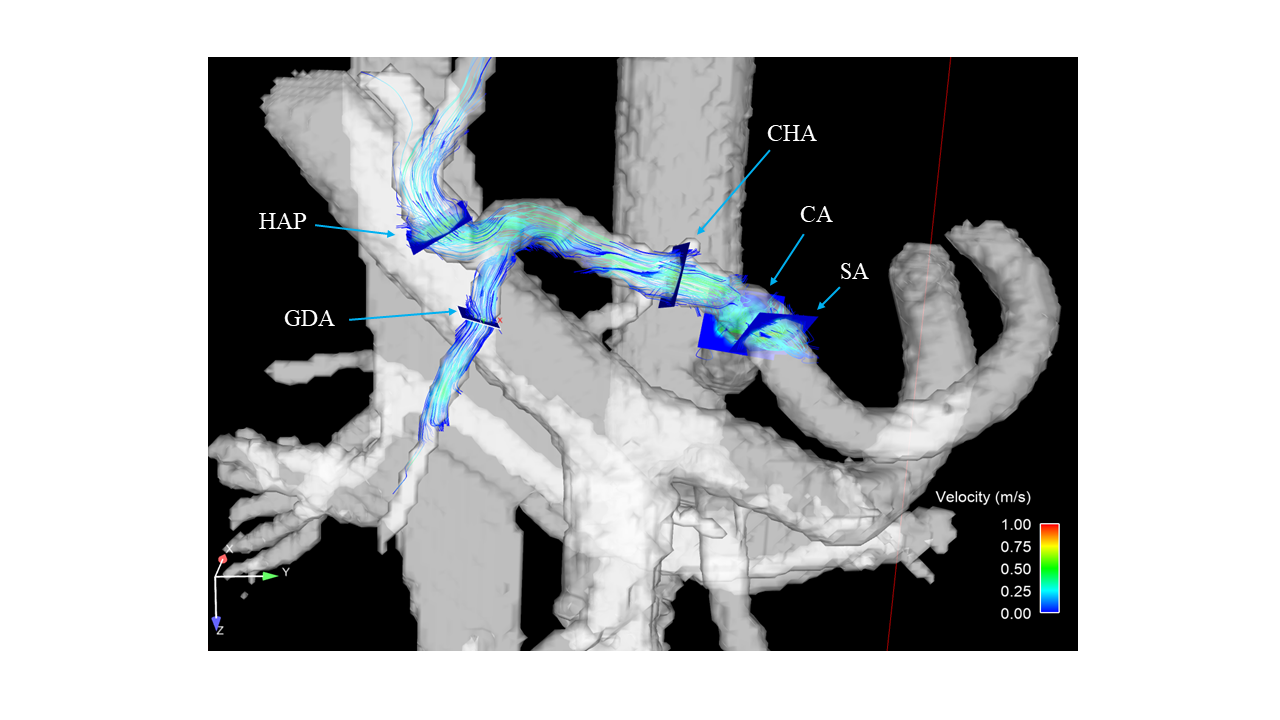
Chronic mesenteric ischemia (CMI) is a rare disease caused by reduced blood flow to the intestines, most often from atherosclerotic lesions existing in proximal segments of mesenteric vasculature1. Due to the extensive collateralization of the mesenteric arteries, at least 2 of the 3 main mesenteric arteries (namely, superior mesenteric (SMA), celiac (CA), and inferior mesenteric artery (IMA)) must be compromised before symptoms are seen in most cases1. The pancreaticoduodenal arcade (PDA) is a primary collateral network between the SMA and CA2,3, as seen in Figure 1. It is well documented that this pathway serves as a major collateral in patients with celiac stenoses3,4. However, blood flow patterns in this collateral network have not been thoroughly studied in CMI patients due to a lack of suitable tools. This study utilizes 4D flow MRI to quantitatively assess hemodynamics in an arterial segment in the PDA, the gastroduodenal artery (GDA), in controls (N=14) and patients suspected of CMI (N=14) before and after a standardized meal.Methods
In this patient-compliant and IRB-approved study, 20 healthy volunteers (age range 19-73y, mean=44y, females=8) and 19 patients (age range 21-86y, mean=50y, females=14) with a suspicion of mesenteric ischemia were imaged on clinical 1.5T and 3.0T scanners (GE Healthcare, Waukesha, WI). 4D PC-MR data were acquired before and after meal ingestion using radially-undersampled PC-VIPR acquisition5,6 with full volumetric coverage of the upper abdomen: imaging volume: 32x32x24cm spherical; 1.25mm isotropic resolution; TR/TE=6.6-8.3ms/1.9-2.7ms; tip angle=6-15°; Venc=100-120cm/s; intravascular contrast agent (0.03mmol/kg gadofosveset trisodium (Lantheus, N. Billerica, MA)); with retrospective ECG and respiratory gating. Pre-prandial imaging was performed after 5 hours of fasting. After the first scan, subjects orally ingested 474 mL EnSure Plus® (Abbot Laboratories, Columbus, OH) and scanning resumed 20 minutes after ingestion. 3D vessel segmentation from the PC data was performed using Mimics (Materialize, Leuven, Belgium). GDA cut-plane placement and flow visualization was performed in Ensight (ANSYS, Canonsburg, PA). Cut-planes were exported to a customized software package7 for manual temporal segmentation. After data analysis, diagnoses for the patient group were given. The patient group was subdivided into a true CMI group (N=6) and negative diagnosis group (N=13) based on these diagnoses. Flow was compared between each subgroup using a two-tailed Welch t-test. For all statistical tests, p<0.05 was chosen to reflect statistical significance. Effect sizes (Cohen’s d)8 were calculated for each test.Results
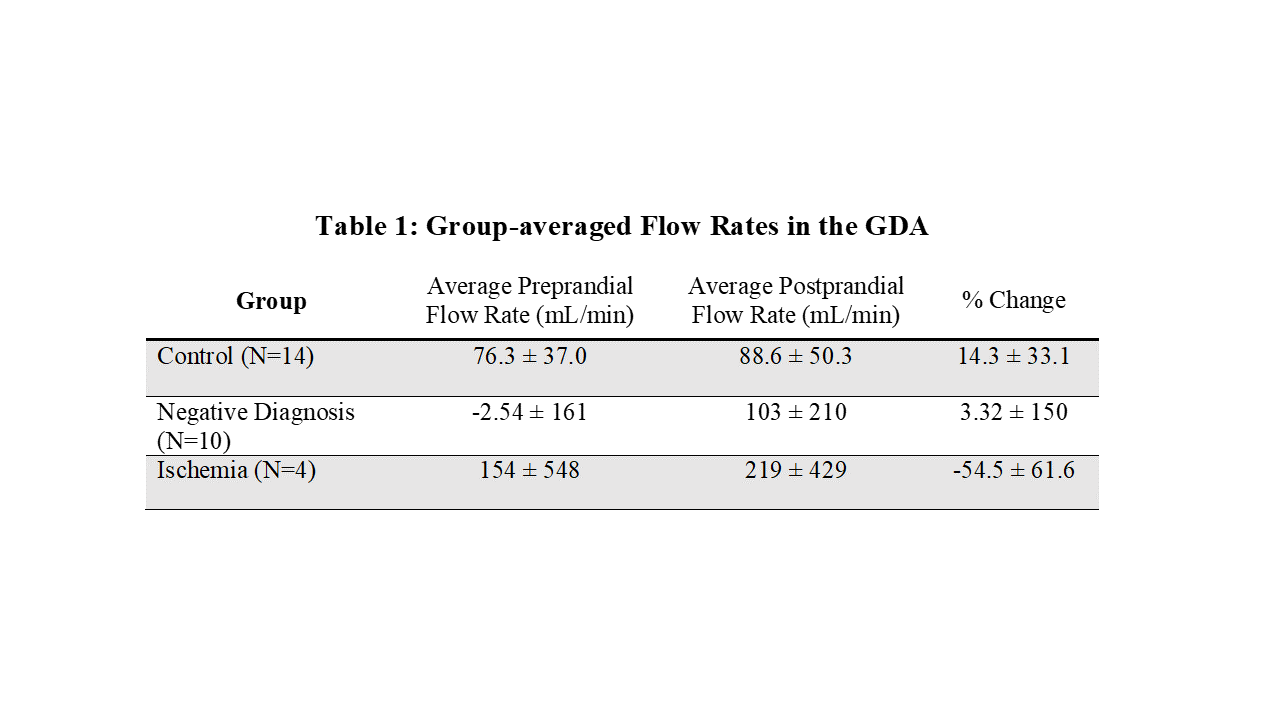
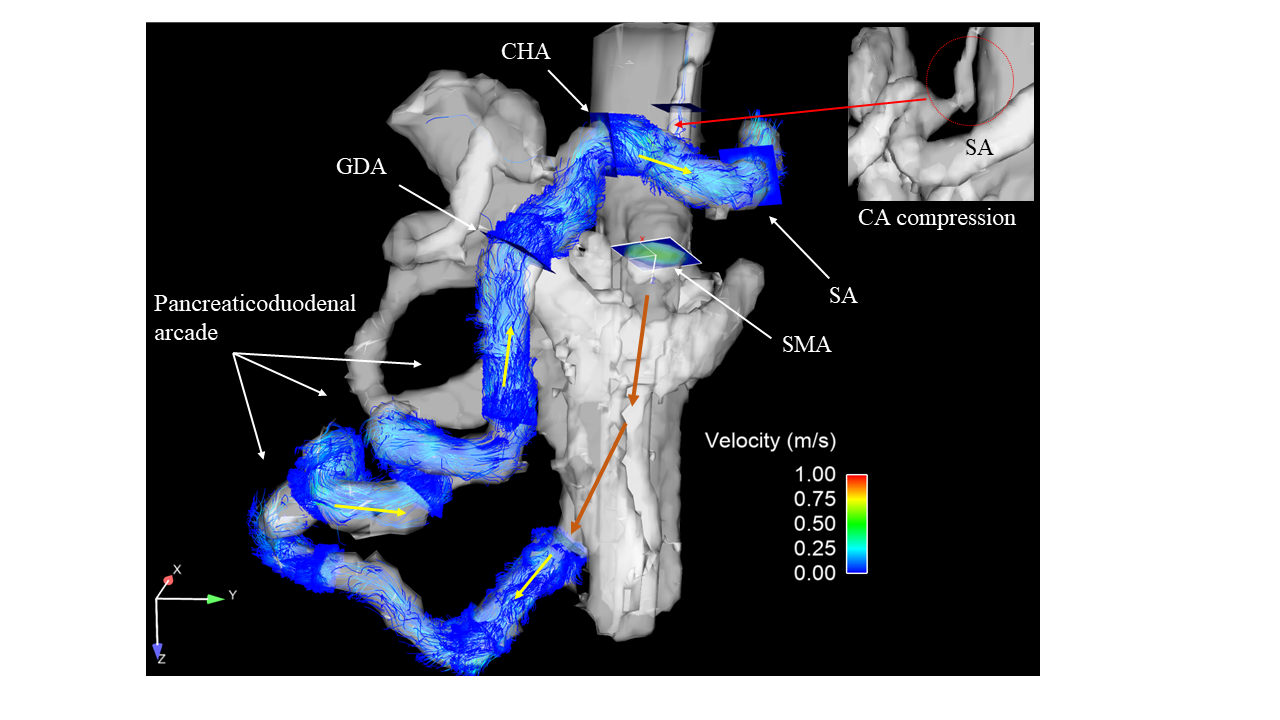
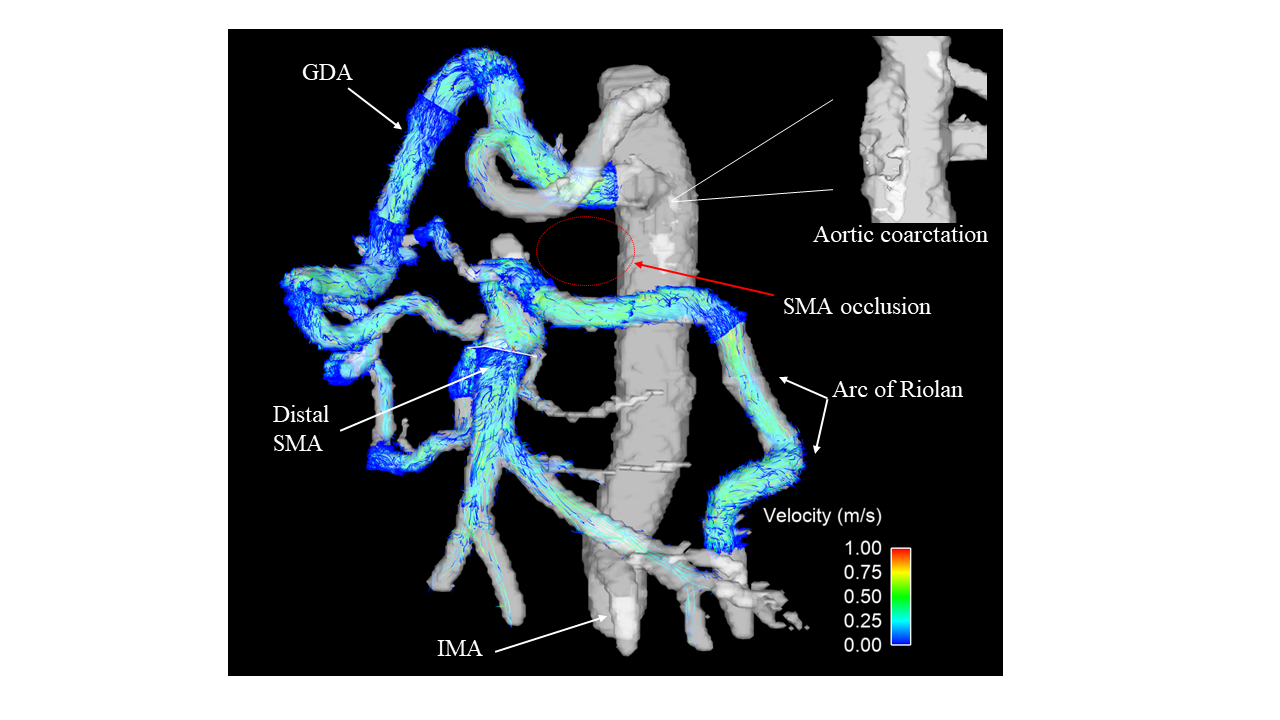
4D flow MRI data were successfully obtained for all 39 subjects; the GDA was visualized in 28 of these patients (14 controls; 10 negative diagnosis; 4 ischemia). From the ischemia group, there were 2 patients with both SMA and CA stenoses (visualized on CT angiography), 1 with median arcuate ligament syndrome (MALS), and 1 with SMA stenosis/aortic coarctation. From the negative diagnosis group, 3 patients had CA narrowing visible on CT angiography and PC-MR angiography (produced from 4D flow data). Average flow rates and percent change in flow values for each group are summarized in Table 1. Results showed no significant difference in preprandial (p=0.796, Cohen’s d=0.199), postprandial (p=0.588, d=0.425), or percent change in flow (p=0.108, d=1.389) between the CMI and control group. Secondly, there was no significant difference in preprandial (p=0.161, d=0.675), postprandial (p=0.838, d=0.093), or percent change in flow (p=0.825, d=0.101) between the negative diagnosis and control group. However, distinct pathology-dependent flow patterns emerged. Specifically, retrograde flow patterns were evident in several negative diagnosis patients with celiac narrowing and a CMI patient with CA compression from MALS (Figure 2). Marked anterograde flow was seen in one CMI patient with SMA stenosis/aortic coarctation (Figure 3) and a negative diagnosis patient with SMA narrowing. Figure 3 shows a CMI patient with an SMA and CA occlusion with pronounced collateral visualization.Discussion
In control subjects, average preprandial, postprandial, and percent change in flow values were relatively stable and almost exclusively anterograde (Figure 4). Flow values and flow responses varied dramatically in both negative diagnosis and CMI patients without any clear anterograde or retrograde bias. However, if grouped by stenosis location, the GDA flow patterns are consistent: (1) retrograde flow existed in patients with celiac narrowing or compression, (2) increased anterograde flow existed in patients with SMA stenosis/narrowing. GDA flow measures might be useful in pinpointing the site of stenoses and/or the hemodynamic significance of such stenoses.Conclusion
In summary, measuring flow patterns in the GDA using 4D flow MRI may provide additional insights into specific disease processes causing CMI. Larger patient cohorts are warranted to verify this finding by allowing sub-categorization based on stenosis location.Acknowledgements
No acknowledgement found.References
1. Sreenarasimhaiah J. Chronic mesenteric ischemia. Best Pract Res Clin Gastroenterol 2005;19:283–295.
2. van Petersen AS, Kolkman JJ, Meerwaldt R, et al. Mesenteric stenosis, collaterals, and compensatory blood flow. J Vasc Surg 2014;60:111–119.
3. Song S-Y, Chung JW, Kwon JW, et al. Collateral Pathways in Patients with Celiac Axis Stenosis: Angiographic–Spiral CT Correlation. RadioGraphics 2002;22:881–893.
4. Poole JW, Sammartano RJ, Boley SJ. Hemodynamic basis of the pain of chronic mesenteric ischemia. Am J Surg 1987;153:171–6.
5. Gu T, Korosec FR, Block WF, et al. PC VIPR: A high-speed 3D phase-contrast method for flow quantification and high-resolution angiography. AJNR Am J Neuroradiol 2005;26:743–749.
6. Johnson KM, Markl M. Improved SNR in phase contrast velocimetry with 5-Point balanced flow encoding. Magn Reson Med 2010;63:349–355.
7. Stalder AF, Russe MF, Frydrychowicz A, Bock J, Hennig J, Markl M. Quantitative 2D and 3D phase contrast MRI: optimized analysis of blood flow and vessel wall parameters. MRM 2008;60:1218–1231.
8. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: L. Erlbaum Associates; 1988.
Figures