1671
Quantitative dynamic contrast-enhanced magnetic resonance imaging as a potential tool for preoperative predicting the response to neoadjuvant chemotherapy in locally advanced gastric adenocarcinoma1Department of Imaging Diagnosis, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 2Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China, 3GE healthcare, China, Beijing, China
Synopsis
Dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) has been applied in diagnosis of different cancers, however its potential in gastric cancer has not been fully explored. In this study, we research into the value of DCE-MRI parameters in evaluating the response to chemotherapy in gastric cancer. It was found that the Ktrans and Ve values showed good predictive performance through distinguishing responders from non-responders, which could provide effective technical assistance for the choice of clinical treatment.
Purpose
To investigate the predictive value of dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) quantitative parameters for the efficacy of neoadjuvant chemotherapy in locally advanced gastric adenocarcinoma (LAGA).Materials and Methods
Sixty-five cases of LAGA (stage II–IVa) confirmed by gastroscopy pathology and received neoadjuvant chemotherapy (NCT) between 2015 and 2017 in the National Cancer Center of China were enrolled in this study. All patients received 4 cycles of SOX NCT, and quantitative DCE-MRI was performed before treatment. The DCE-MRI was performed on 3.0-Tesla MRI scanner (Discovery MR750 3.0 T, GE Medical Systems, Milwaukee, WI, USA) with an 8-channel CTL Target Array Coil. T1 mapping with four different flip angle (3°, 6°, 9°, 12°) and a 42 phases DCE were scanned using LAVA sequence. Quantitative parameters, including volume transfer constant (Ktrans), rate constant (Kep), volume fraction of extravascular extracellular space (Ve) and volume fraction of plasma (Vp), were calculated by the Extended-Toffs model on an in-house developed software, Omni Kinetics 2.0.10 (Life Science, GE Healthcare, China). After NCT, all patients received radical gastrectomy. According to postoperative Mandard pathological tumor regression grade (TRG), patients were divided into responders (TRG 1-3) and non-responders (TRG 4, 5). The clinical pathological features were recorded. The differences of clinical pathological features and pretreatment DCE quantitative parameters between the two groups were compared by t test, Mann-Whitney U test, χ2 test or Fisher exact probability, depending on the data type. The diagnostic performance of different parameters was judged by the receiver-operating characteristic curve (ROC) analysis. ROC curve was utilized to analyze the predictive efficacy of DCE quantitative parameters for NCT response of LAGC, and multivariate logistic regression analysis was performed to analyze the predictive efficacy of combined parameters.Results
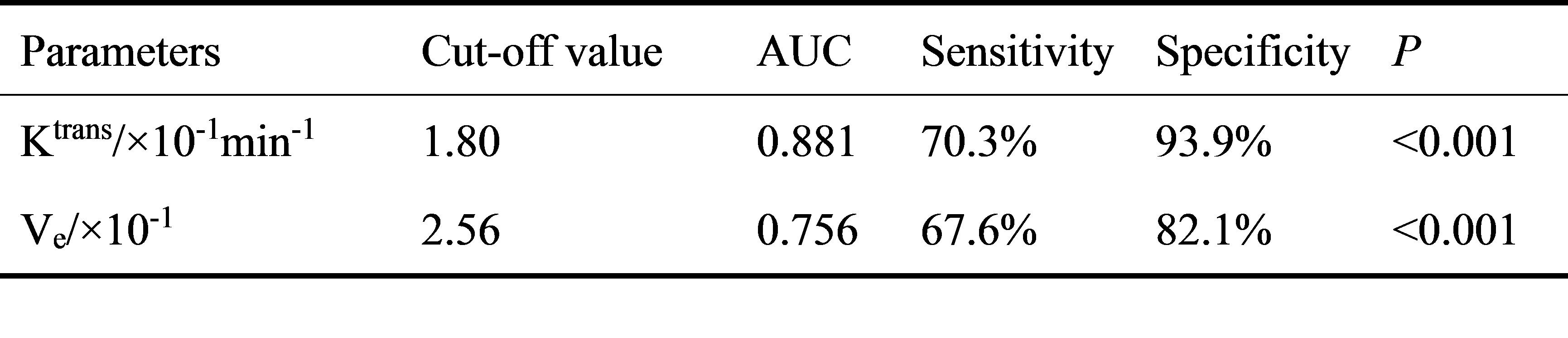
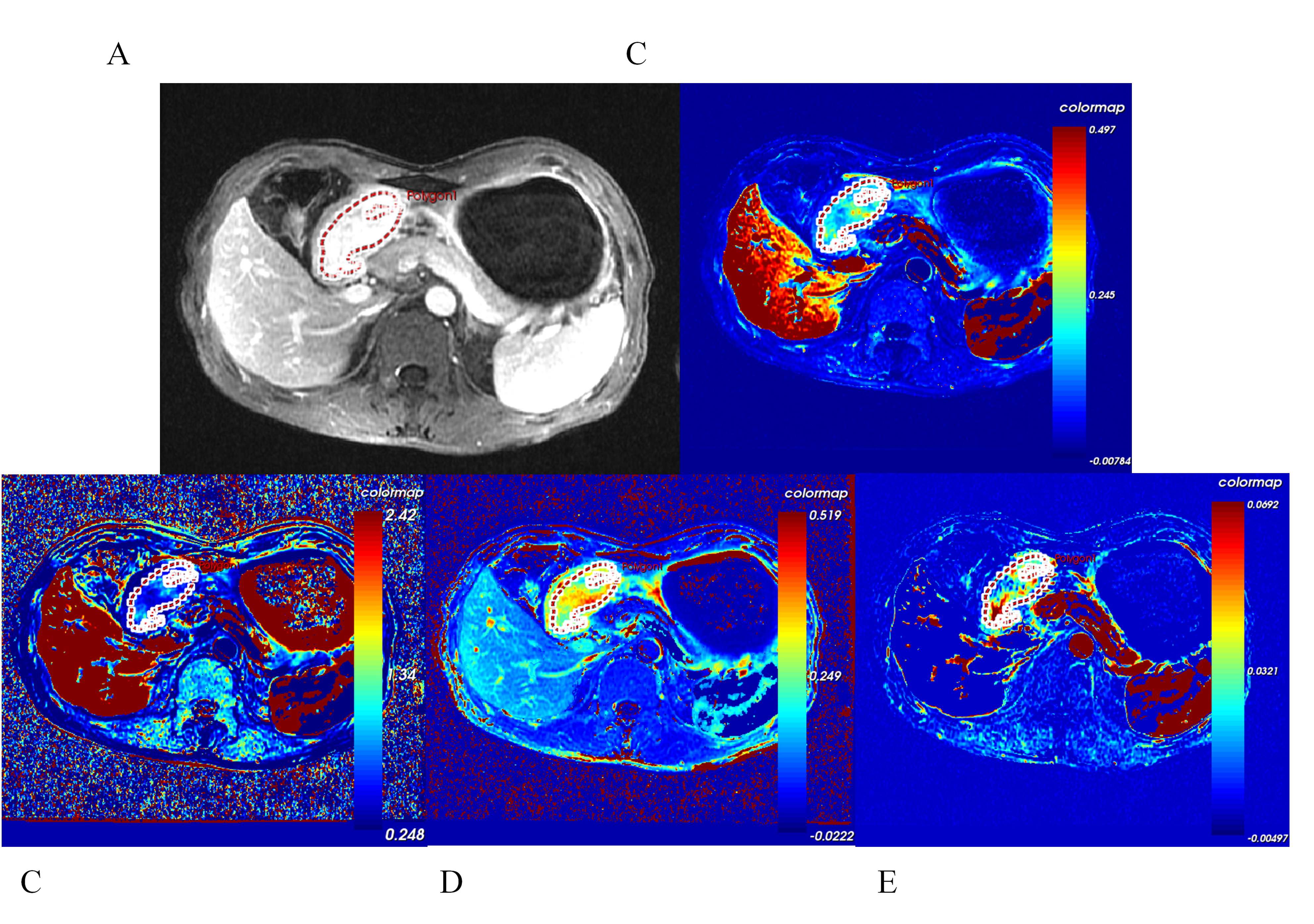
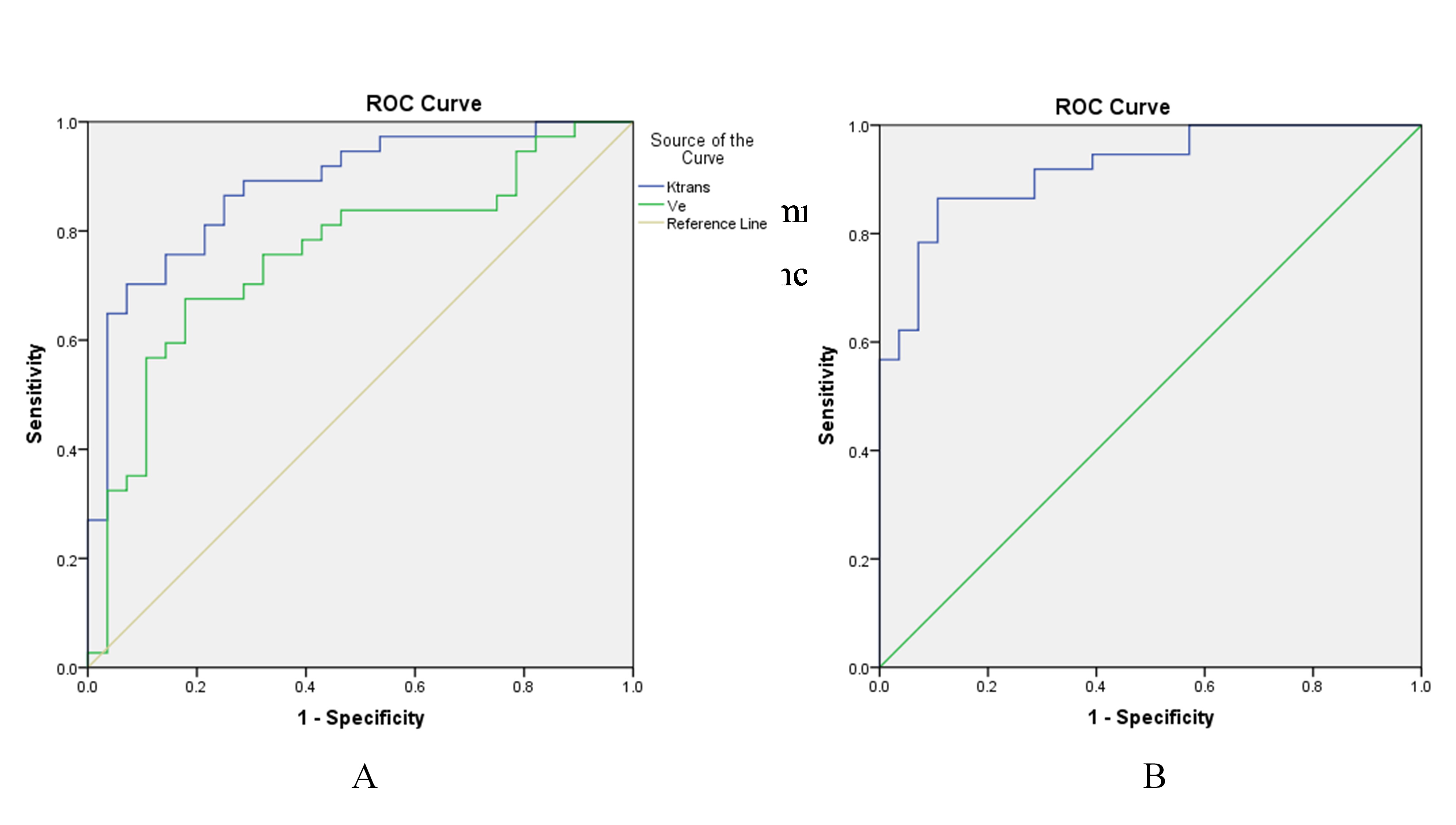
Based on the Mandard TRG criteria after 4 cycles of NCT, 37 patients were categorized into the responder group (Figure 1) whereas the other 28 patients were considered non-responders group. No significant difference was found in clinicopathologic features (All P>0.05) (Table 1). The pretreatment Ktrans and Ve values were significantly higher in the responders than non-responders (P<0.001) (Table 2), Kep was higher in responders than non-responders (P=0.10), but the difference did not showed statistically significant. Vp showed no statistical difference between the two groups (P>0.05). ROC analysis (Figure 2) showed the AUC of Ktrans and Ve values predicting NCT efficacy were 0.881 and 0.756 respectively, the corresponding cut-off value, sensitivity and specificity were displayed in Table 3. Multiple logistic regression analysis showed that the combination of the two parameters could improve the AUC up to 0.921, with the sensitivity and specificity of 86.5% and 89.3%, respectively (Figure 2).Discussion
NCT is an important part of comprehensive treatment of gastric cancer nowadays, but the response to neoadjuvant therapy is highly individual [1]. Predicting tumor response to chemotherapy as accurate as possible could help determine an optimal treatment regimen and have considerable clinical benefits for LAGA patients. However, there was no widely accepted curative effect prediction standard of NCT in gastric cancer [2]. The RECIST, a widely adopted standard for evaluating therapy response based on the change in tumor size, is restricted in gastric cancer, since the stomach is a cavity viscera. Recently, quantitative DCE-MRI showed promising potential for preoperative noninvasive prediction and assessment of curative effects in a variety of tumors [3]. In this study, pretreatment Ktrans was significant higher in responders, which represented the microvascular permeability within the tumor bed. This suggests that a more permeable tumor neovasculature may provide better access for chemotherapy compared with less permeable, less well-vascularized tumors [4]. We found the Ve value was significantly significant higher in responders, which may be due to the need for a sufficient extracellular space volume of distribution for chemotherapy to efficiently kill tumor cells and for oxygen to distribute efficiently throughout the tumor to avoid significant hypoxia. Kep was higher in responders, but no significant difference was observed, which may be due to the small sample size. Vp showed no statistical difference between the two groups, which was rarely reported in the previous literature. Further study was needed to clarify the meaning of Vp.Conclusion
DCE-MRI quantitative parameters, especially the Ktrans and Ve values, could help to predict the NCT response of LAGA, and the combination of parameters could improve the predictive efficacy.Acknowledgements
This study was supported by the Beijing Hope Run Special Fund of Cancer Foundation of China (LC2016A06).References
[1] Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006 Jul 6;355(1):11-20.
[2] Robb WB, Mariette C. Predicting the response to chemotherapy in gastric adenocarcinoma: who benefits from neoadjuvant chemotherapy? Recent Results Cancer Res. 2012;196:241-68.
[3] Tofts PS, Brix G, Buckley DL, et al. Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging. 1999 Sep;10(3):223-32.
[4] Tong T, Sun Y, Gollub MJ, et al. Dynamic contrast-enhanced MRI: Use in predicting pathological complete response to neoadjuvant chemoradiation in locally advanced rectal cancer. J Magn Reson Imaging. 2015 Sep;42(3):673-80.
Figures
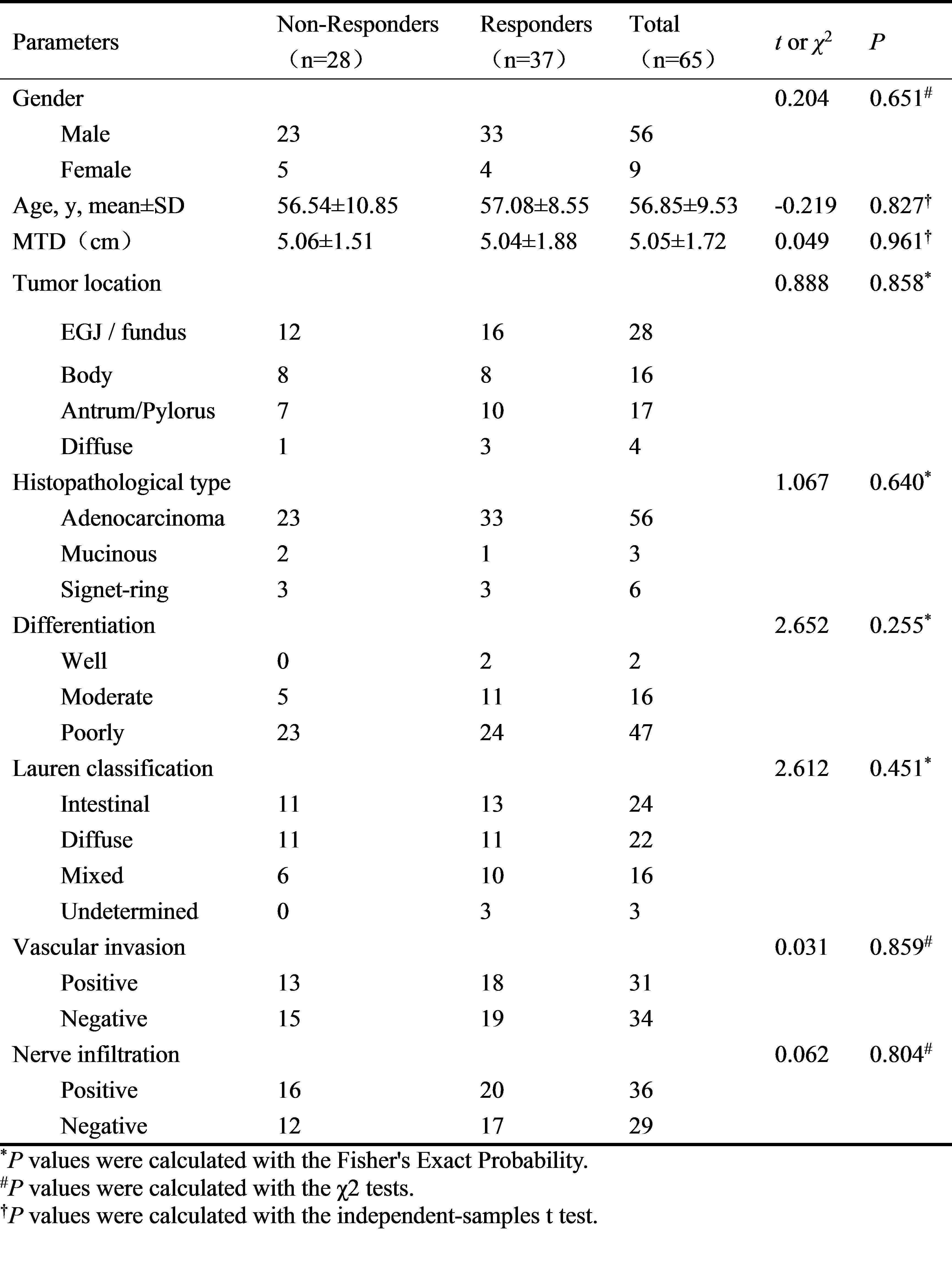
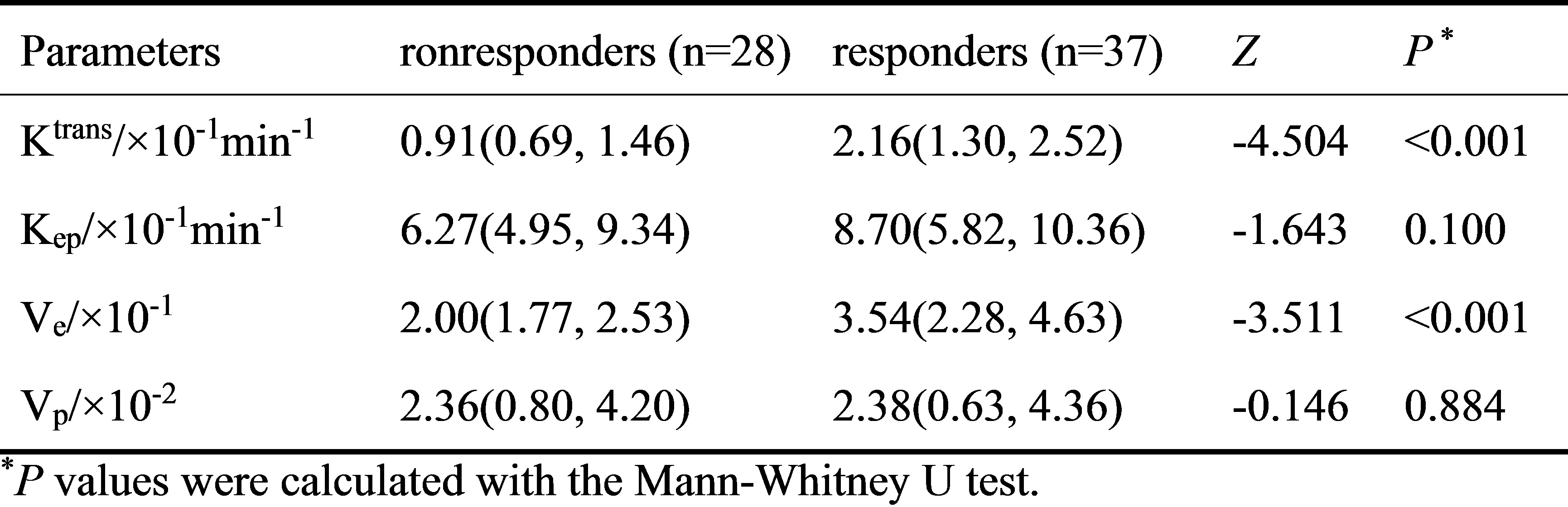
Table 2. Comparison of pretreatment quantitative DCE-MRI parameters between responders and non-responders groups