1670
Robust Breath-hold Three-Dimensional (3D) MRCP using Contrast-Enhanced Timing Robust Acquisition Order with a Preparation of the Longitudinal Signal Component(CENTRA-Plus) Technique at 3TYoshihiro Ikeda1, Yasuhiro Goto1, Masami Yoneyama2, Isao Shiina1, Yutaka Hamatani1, Kazuo Kodaira1, Yu Nishina3, Satoru Morita3, and Shuji Sakai3
1Department of Radiological Services, Tokyo Women's Medical University Hospital, Tokyo, Japan, 2Philips Electronics Japan, Tokyo, Japan, 3Department of Diagnostic Imaging and Nuclear Medicine, Tokyo Women's Medical University Hospital, Tokyo, Japan
Synopsis
The present study investigates the clinical utility of motion-insensitive breath-hold 3D MRCP using contrast-enhanced timing robust acquisition order with a preparation of the longitudinal signal component(CENTRA-Plus). 3D MRCP image derived from breath0holding with CENTRA-Plus showed good correlations to those from conventional respiratory triggering technique. Breath hold 3D MRCP with CENTRA-Plus can reduce scan time (around 80% of the scan time) without any penalty for the image quality; therefore, it might contribute to great advantages in routine clinical work.
Purpose
Breath-hold MRCP has recently gained more attention in routine clinical MRI, but its limited scan time during the breath-hold period often results in poor signal-to-noise ratio (SNR) and spatial resolution. We may be able to obtain higher SNR images with longer scan times, but such protocol is unrealistic and reduces the success rate of the examination in case of incomplete breath-holding. The situation of an incomplete breath-hold that the failure of the breath-hold should occur in the latter half of the scanning. We applied a unique k-space ordering called contrast enhanced timing robust acquisition order with a preparation of the longitudinal signal component (CENTRA-Plus), which has been originally applied to contrast enhanced abdominal imaging [1], to improve the image quality of breath hold MRCP. Our hypothesis is that the CENTRA-Plus may be tolerable for such fail in breath-hold, which happens in the latter half of the scanning. The purpose of this study was to demonstrate the advantage of CENTRA-Plus over the conventional method.Method
In CENTRA-Plus k-space ordering, k-space is basically segmented by two (central and peripheral) sectors in the Ky and Kz directions. Actual data acquisition is started from the central k-space sector with a linear profile-ordering acquisition in individual shots and then moves out toward peripherally within the central k-space sector. After the complete filling of the central sector, data acquisition is then continued toward peripheral k-space with a quasi-elliptical centric profile-ordering scheme. With CENTRA-Plus, acquisition is started in the central k-space sector and the most central k-space sector is acquired at an early stage. Thus, we hypothesized that this technique may be less affected by motion on the latter half of the imaging time. 3D MRCP images with six healthy volunteers (six male, age range: 25-42 years) were obtained by 3.0T MR system (Ingenia, Philips healthcare). We compared three types of 3D MRCP images: conventional 3D turbo spin echo (TSE) respiratory triggering technique, 3D breath holding gradient and spine echo(GRASE), 3D TSE breath holding CENTRA-Plus. As a quantitative evaluation, the contrast ratio of the common bile duct to the liver and the signal-to-noise ratio (SNR) of the common bile duct were calculated. Qualitative analyses on an overall image quality, sharpness and signal of common bile duct on a 4-point scale scored by 2 independent radiologists were compared using Wilcoxon signed-rank test.Result&Discussion
Figure 1 shows representative MRCP images obtained from conventional method and CENTRA-Plus method. No significant differences in the SNR between conventional method and CENTRA-Plus (18.2±9.2 vs. 12.3±5.1,[e1] p = 0.29) and between GRASE and CENTRA-Plus (22.9±16.6 vs. 12.3±5.1,[e2] p = 0.17) were observed. No significant differences in the CR between conventional method and CENTRA-Plus (0.9±0.02 vs. 0.9±0.02, p= 0.06) and between GRASE and CENTRA-Plus (0.9±0.04 vs. 0.9±0.02,[e3] p = 0.68) were observed. No significant differences in the overall image quality between conventional method and CENTRA-Plus (3.1±0.4 vs. 3.0±0.6, p = 0.67) and between GRASE and CENTRA-Plus (3.2±0.41 vs. 3.0±0.63, p = 0.67) were observed. The average scan time for conventional respiratory triggering method and breath-hold CENTRA-Plus was 2 minutes 30 seconds and 18 seconds, respectively. Breath-hold CENTRA-Plus can shorten about 80% of the scan time for conventional method. Use of CENTRA-Plus was possible to obtain good image quality without motion artifacts despite the incomplete breath-holding (Figure.2).Acknowledgements
No acknowledgement found.References
[1] Beck GM, De Becker J, Jones AC, von Falkenhausen M, Willinek WA, Gieseke J. Contrast-enhanced timing robust acquisition order with a preparation of the longitudinal signal component (CENTRA Plus) for 3D contrast-enhanced abdominal imaging. J Magn Reson Imaging. 2008;27:1461-7.Figures
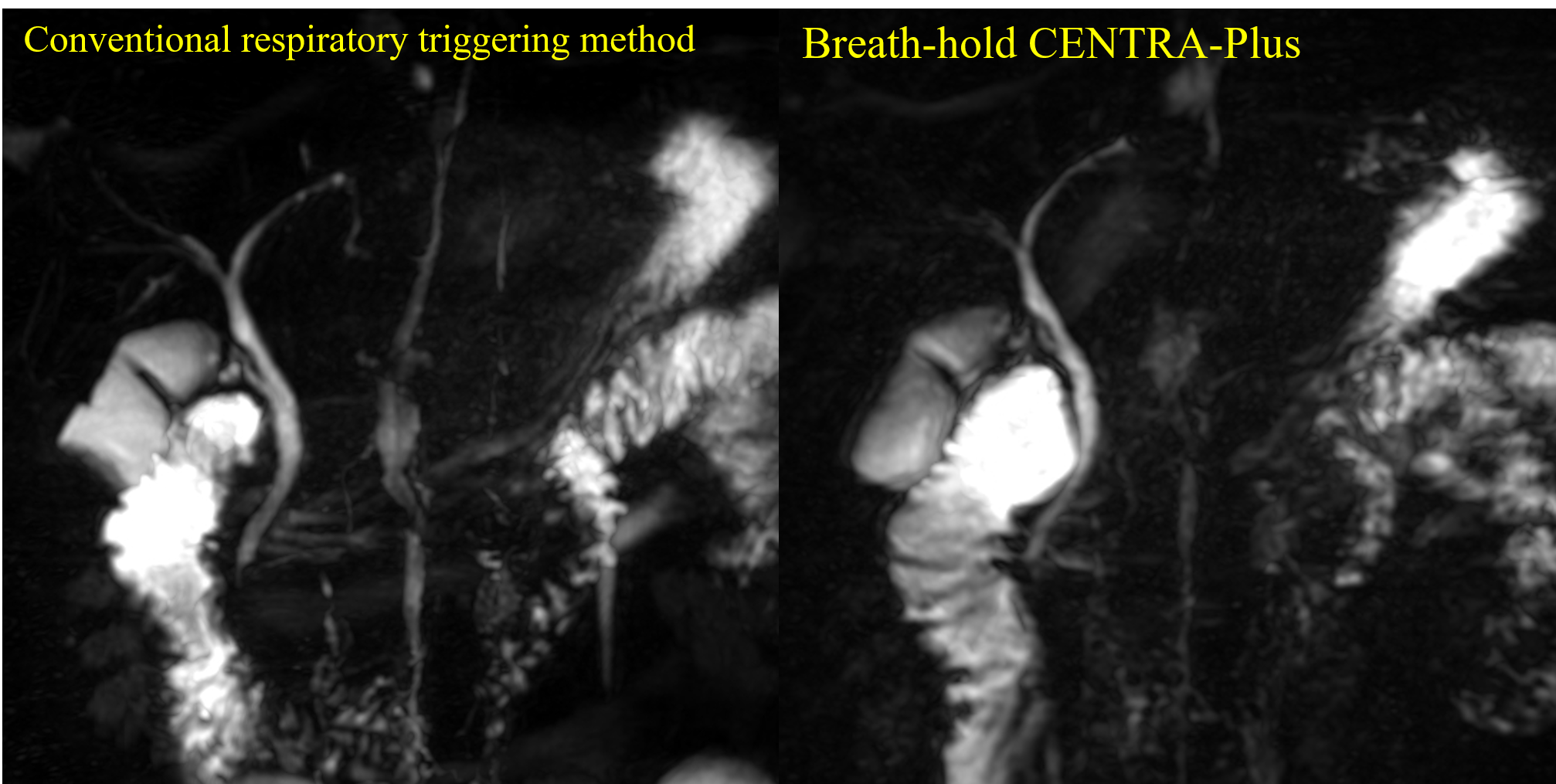
Figure 1: Conventional respiratory triggering method, breath-hold CENTRA-Plus. Acquisition time was 2 minutes 30 seconds for conventional respiratory triggering method, and 18 seconds for breath-hold CENTRA-Plus.
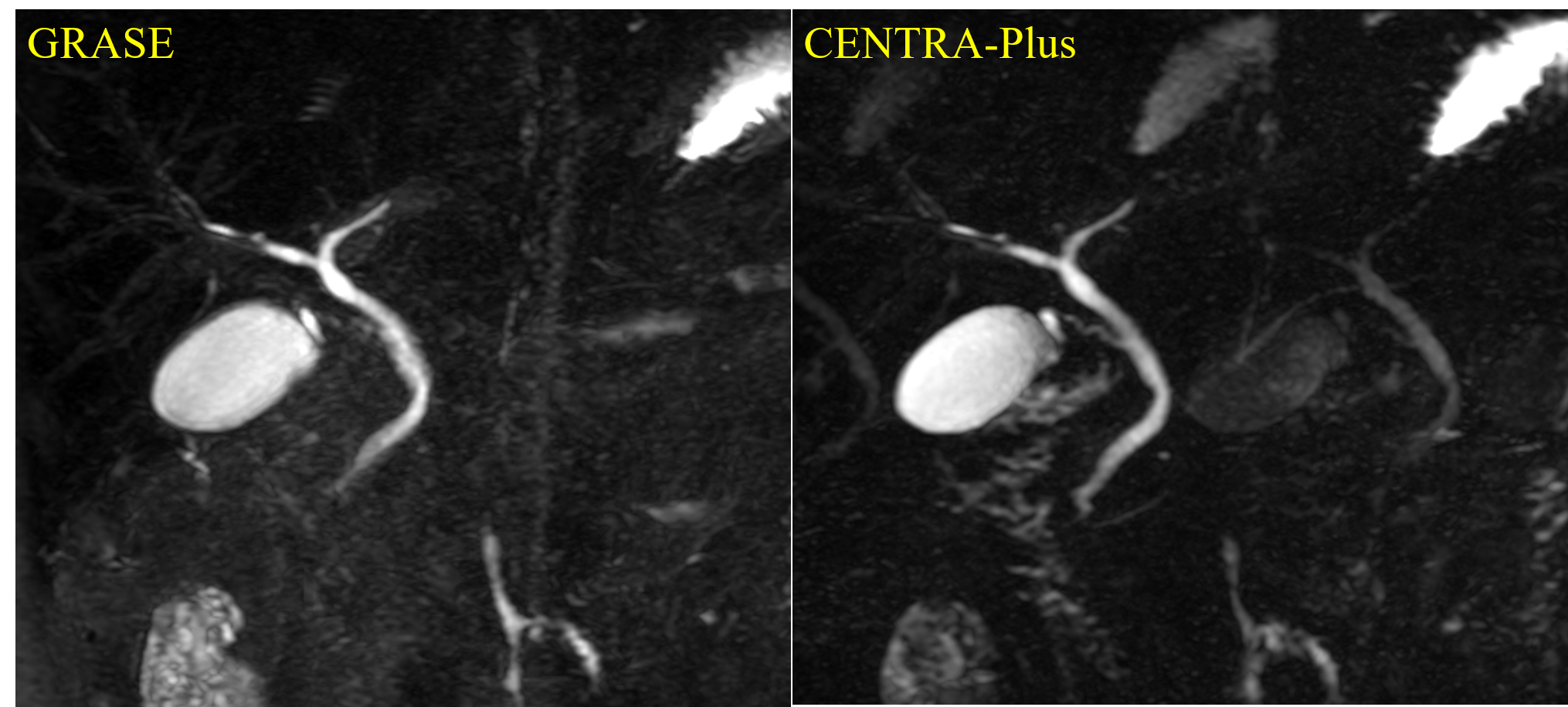
Figure 2:Incomplete breath-holding GRASE and CENTRA-Plus