1666
Differentiation of Pancreatic Head Ductal Adenocarcinoma from Inflammatory Pancreatic Pseudomass by MR Cholangio-pancreatography: Utility of the Duct-interrupted, Corona and Attraction Signs1Division of Body MRI, Department of Radiology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States, 2Department of Radiology, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, United States
Synopsis
To properly treat and determine a truthful prognosis, accurate pancreatic head mass differentiation is fundamental. Pancreatic ductal adenocarcinoma (PDAC) of the head and inflammatory pancreatic pseudomass (IPP) simulate significantly to each other in clinical imaging. We proposed the use of three radiological signs ("duct-interrupted”, “
Introduction
Accurate differentiation between inflammatory pancreatic pseudomasses (IPP) and pancreatic ductal adenocarcinoma (PDAC) is fundamental to a patient’s management and prognosis. Radiologists may often encounter lesions that distort the normal contour of the pancreatic head, simulating the appearance of pancreatic cancer, but without any of the pathognomonic features to confirm the diagnosis. In the absence of or prior to histopathological confirmation, differentiation between IPP and PDAC by imaging diagnosis may play a significant role in the management of these patients, especially since the treatment choice may range from invasive surgical resection for PDAC to pharmacological management for IPP [1, 2]. Although magnetic resonance cholangio-pancreatography (MRCP), in the setting of pancreatic mass evaluation is already widely used, only few studies have shown the utility and specificity of MRCP in this context [3-5].Therefore, the purpose of our study is to determine the utility of three MRCP signs, the “duct-interrupted”, “corona” and “attraction” signs for the differentiation of PDAC from IPP in the pancreatic head.Materials and Methods
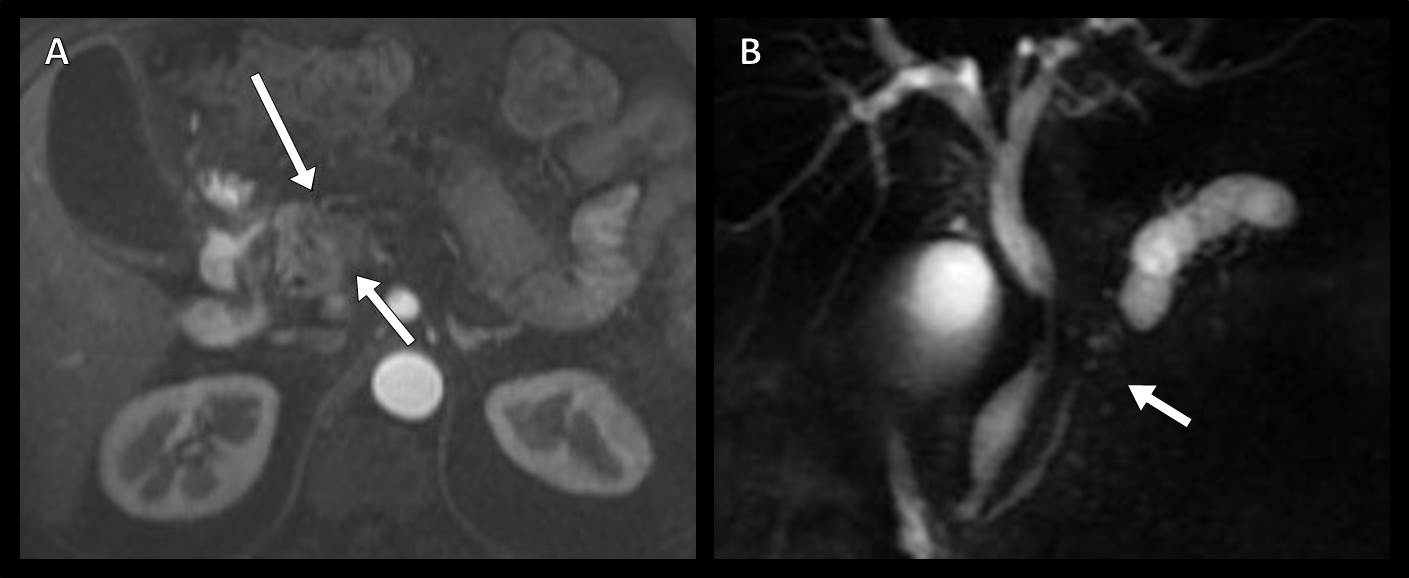
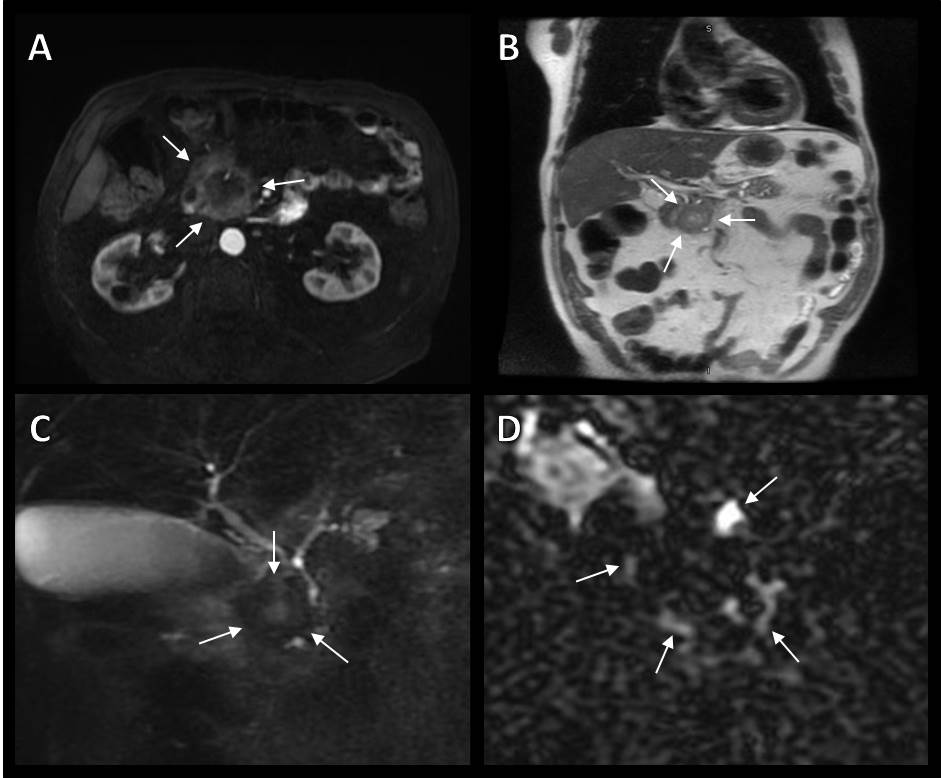
This HIPAA-compliant, institutional review board-approved retrospective study with written consent waived included 53 adults (33 men and 20 women, mean age, 55 years; range, 17-87 years) with a pancreatic head mass who underwent MRCP. Final diagnosis was established by means of histopathology, serum IgG4 levels, and/or reduction of at least 50% of size/complete resolution of mass at follow-up. Three blinded radiologists independently reviewed each MRCP exam and three signs were assessed: 1) the “duct-interrupted” sign, deemed positive for PDAC if the duct within the mass demonstrated complete interruption with upstream dilation; 2) the “corona” sign, considered positive for PDAC if dilated side-branches were located exclusively outside the mass; and 3) the “attraction” sign, deemed positive for IPP if the dilated common bile duct showed attraction and angulation towards the mass. Sensitivity, specificity and positive and negative predictive values of the signs in differentiating between IPP and PDAC were calculated, as well as the degree of interobserver agreement, using the chance-corrected κ statistic.Results
Out of 53 masses, 17 (32%) were PDAC and 36 (68%) were IPP. Sensitivity, specificity and positive and negative predictive values of the “duct-interrupted” sign to differentiate between PDAC from IPP for the three readers were 29%-53%, 89%-95%, 56%-82% and 73%-81%, respectively (κ=0.41); for the “corona” sign, they were 29%-53%, 81%-100%, 56%-100% and 75%-78%, respectively (κ=0.4), and for the “attraction” sign, they were 20%-25%, 71%-82%, 64%-75% and 31%-34%, respectively (κ=0.54).Conclusion
The “duct-interrupted” and “corona” MRCP signs have high specificity for diagnosing PDAC while the “attraction” sign has good specificity for identifying IPP.Acknowledgements
No acknowledgement found.References
1. Abraham Susan,Wilentz Robb, Yeo Charles, Sohn Taylos, Cameron John, Boitnott John HR. Pancreaticoduodenectomy (Whipple Resections) in Patients Without Malignancy Are They All “Chronic Pancreatitis”? [Internet]. American Journal of Surgical Patholology. 2003 [cited 2018 Jan 10]. p. 110–20.
2. Kennedy T, Preczewski L, Stocker SJ, Rao SM, Parsons WG, Wayne JD, et al. Incidence of benign inflammatory disease in patients undergoing Whipple procedure for clinically suspected carcinoma: a single-institution experience. [cited 2018 Jan 10]
3. Neff CC, Simeone JF, Wittenberg J, Mueller PR, Joseph Ferrucci IT. Inflammatory Pancreatic Masses Problems in Differentiating Focal Pancreatitis from Carcinoma’. [cited 2018 Jan 10]
4. Lammer J, Herlinger H, Zalaudek G, Hofler H. Pseudotumorous Pancreatitis. Gastrointest Radiol [Internet]. 1985 [cited 2018 Jan 10];10:59–67
5. Kim HJ, Kim YK, Jeong WK, Lee WJ, Choi D. Pancreatic duct “Icicle sign” on MRI for distinguishing autoimmune pancreatitis from pancreatic ductal adenocarcinoma in the proximal pancreas. Eur Radiol. 2015;25(6):1551–60.
Figures