1659
Pancreatic and hepatic iron predict prediabetes in chronically transfused patients with sickle cell disease.1Pediatrics, Children's Hospital Los Angeles, Los Angeles, CA, United States
Synopsis
Pancreatic iron is common in transfused sickle cell disease(SCD) patients but the functional significance is unknown. We compared pancreatic function with hepatic and pancreatic iron burden by MRI in 28 SCD patients. Six patients had impaired fasting glucose(IFG) values and one had impaired glucose tolerance. Insulin resistance was positively associated with body mass index and negatively associated with liver iron concentration (r2 = 0.50, p<0.004). Liver iron and serum ferritin predicted IFG with an AUROC of 0.82 and 0.86 respectively. Beta cell function was inversely proportional to pancreatic R2* (r2 = 0.17, p=0.01). Thus, prediabetic changes were common and related to liver and pancreatic iron.
Introduction
Patients with sickle cell disease (SCD) may require lifelong transfusions for prevention of stroke or acute chest syndrome, leading to iron overload in the liver and spleen. SCD patients are partially protected against endocrine and cardiac complications because they are continually regenerating new red blood cells, lowering their transferrin saturation 1-3. Nonetheless, we have previously demonstrated that this protection can be overwhelmed by sustained transfusion exposure4,5; by the age of 30, more than 50% of chronically transfused SCD patients will have detectable pancreatic iron5. However, to date, no one has explored the functional significance of pancreatic iron in SCD patients. We hypothesized that although SCD patients have a delayed onset of pancreatic iron deposition compared to thalassemia patients, they ultimately demonstrate impaired insulin sensitivity and secretion similar to thalassemia major6.Methods
Patients were recruited from the Hematology clinic at Children’s Hospital Los Angeles. Study was approved by the Committee on Clinical Investigation (CCI#2014-00034) and all patients provided informed consent. Twenty-eight patients with sickle cell disease underwent quantification of liver iron and pancreatic R2* at 1.5 Tesla (Philips Achieva running system 5.1.9) and assessment of fasting glucose and insulin; 9 patients underwent repeat examinations more than 1 year apart for a total of 39 examinations. Liver and pancreatic iron were quantitated using multiple echo, gradient echo acquisitions as previously described and validated by our laboratory 6,7. Twenty-six patients successfully completed a 3 hour oral glucose tolerance test using an 1.75 g/kg glucose dose (max 75 grams). American Diabetes Association criteria were used to score the oral glucose tolerance test results6. Fasting insulin and glucose results were converted to Homeostatic Modeling (HOMA) insulin resistance and beta cell secretion indices using the following relationships8
HOMAIR = (Glucose x Insulin)/405, HOMAβ = 360 x Insulin /(Glucose – 63) [1]
Results
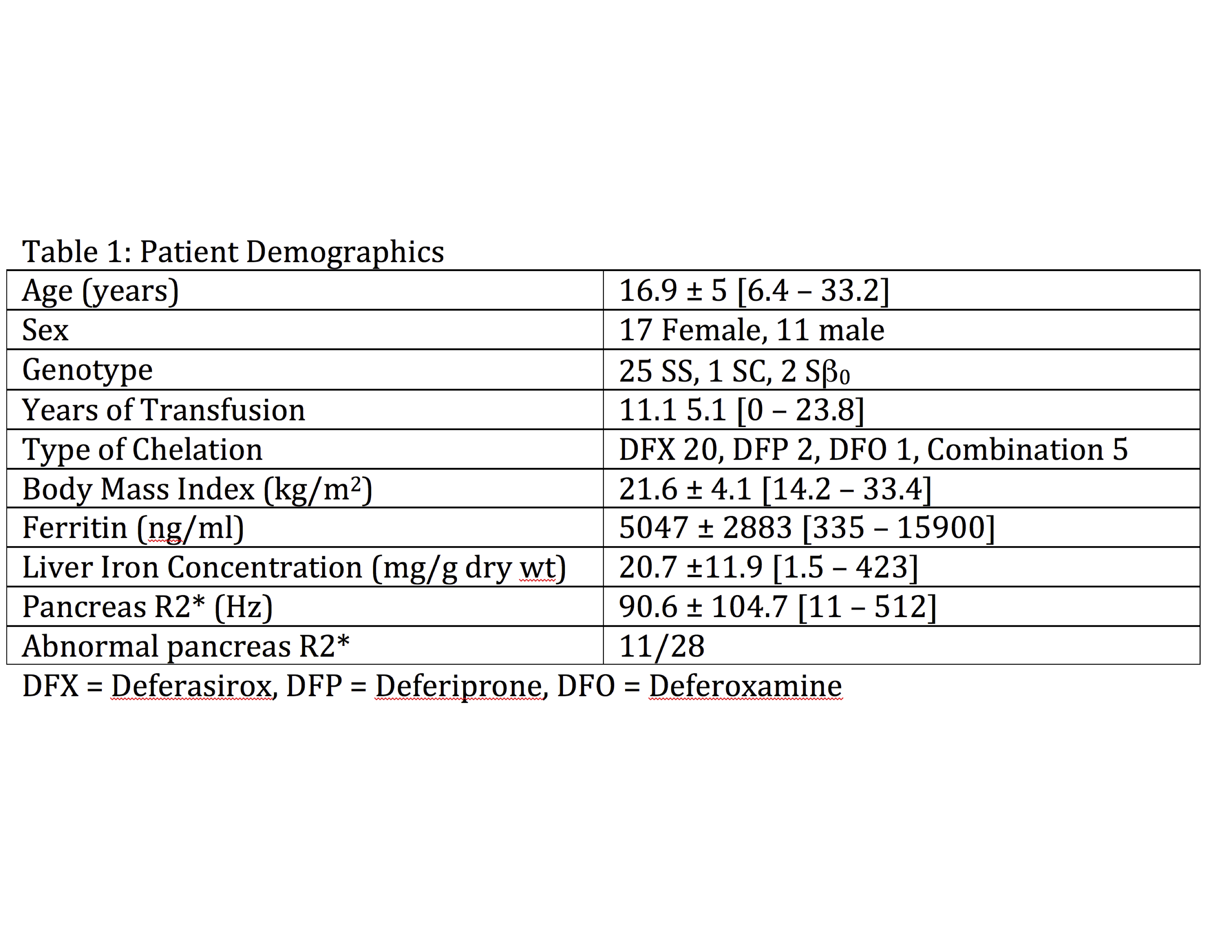
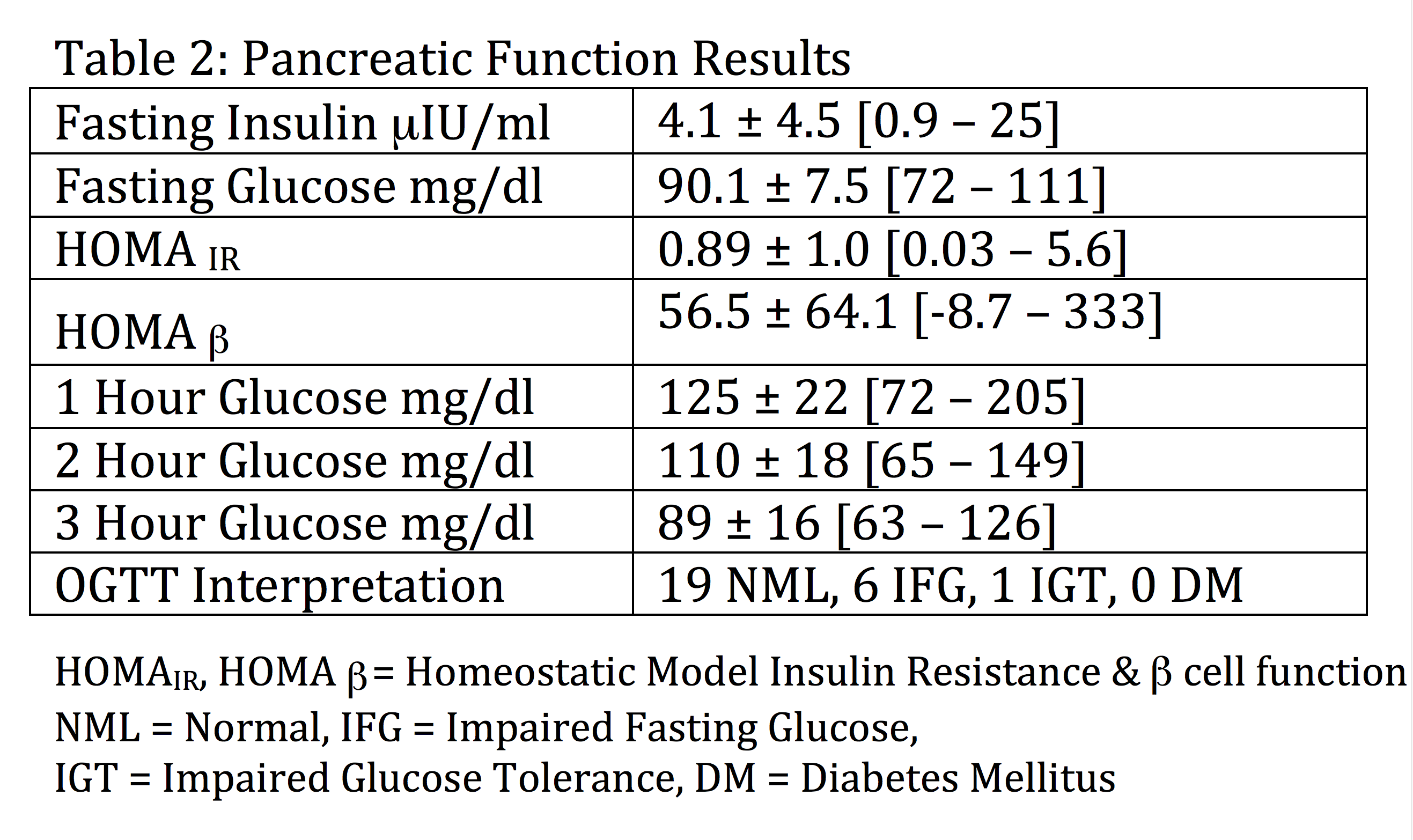
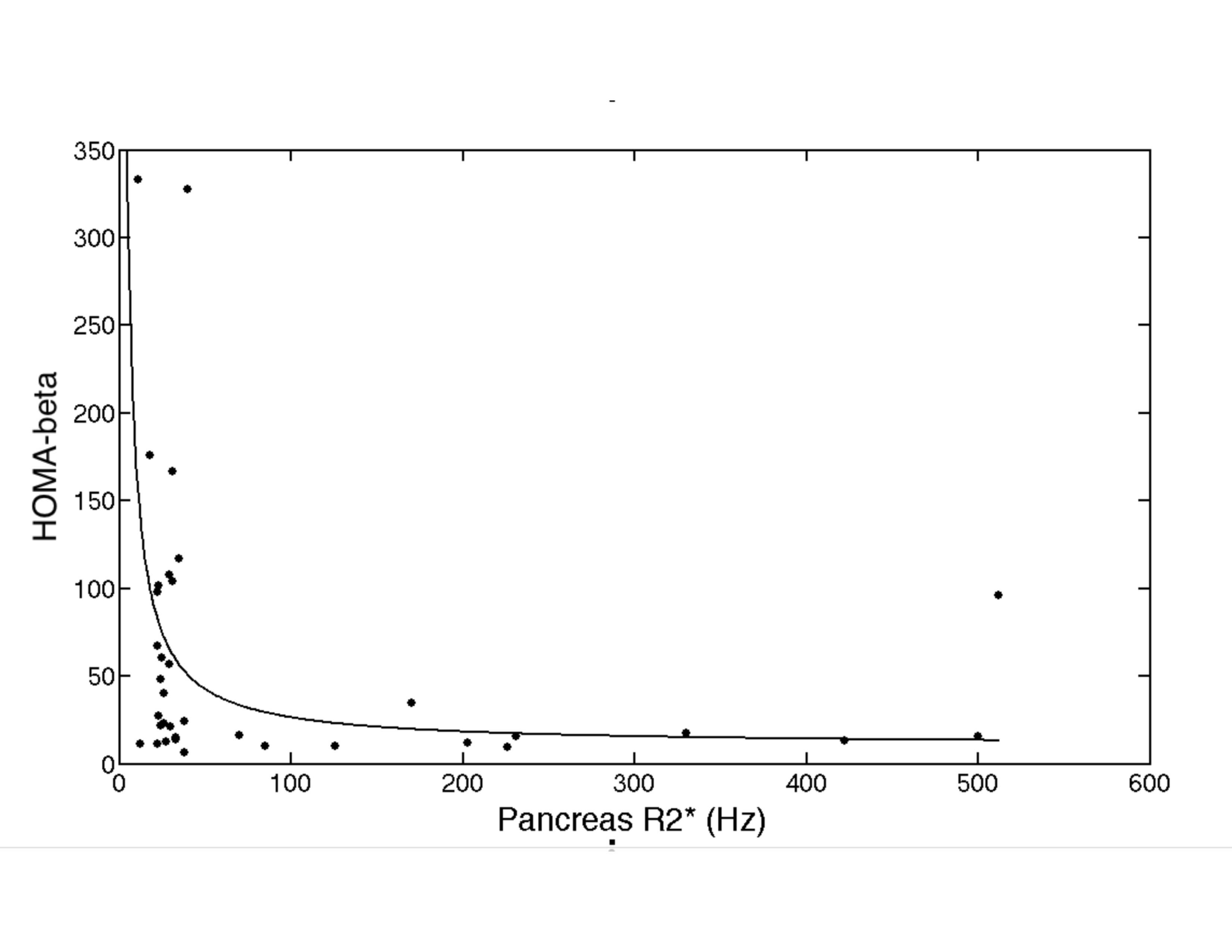
Patient demographics are summarized in Table 1. The patients were mostly children and young adults and relatively balanced with respect to sex. The cohort had severe hepatic siderosis and 11/28 had documented pancreatic siderosis. Table 2 summarizes the pancreatic function studies. Six patients have impaired fasting glucose values and one patient had impaired glucose tolerance. No patient was frankly diabetic. On logistic regression, both liver iron concentration and serum ferritin (but not pancreatic R2*) predicted impaired fasting glucose with AUC’s of 0.82 and 0.86, respectively, and the optimal cutoffs were 22.5 mg/g and 5410 ng/l, respectively. On multivariate analysis, HOMAIR was positively associated with BMI (p=0.0004) and negatively associated with LIC (p=0.004), for a combined r2 of 0.50. Figure 1 demonstrates that HOMAβ varies inversely with pancreatic R2* (r2 = 0.17, p=0.01). The relationship was nearly dichotomous with HOMAβ being significantly lower (20.6 ± 27 vs 78.1 ± 91.3, p = 0.008) in patients having detectable pancreatic iron (R2* > 40 Hz).
Discussion
Pancreatic siderosis was relatively common in our cohort of chronically transfused SCD patients (39%), however the toxicity was relatively mild, consisting of six patients with impaired fasting glucose and one patient with impaired glucose tolerance. This most likely reflects the younger age and the lower duration of transfusional exposure in the present study than our previously reported thalassemia cohort6. LIC and serum ferritin were better predictors of impaired fasting glucose than pancreatic R2*, reinforcing the importance of the liver in glucose homeostasis. Paradoxically, increasing LIC was associated with improved insulin resistance, perhaps by stimulating insulin re-uptake by the liver. While pancreatic iron deposition was not associated with clinical glucose dysregulation, HOMAβ secretion index was dramatically lower in SCD patients with pancreatic iron deposition. Thus we speculate that SCD patients having pancreatic iron deposition are at increased risk for overt diabetes in the future, similar to non SCD patients with abnormal HOMAβ 8, although longitudinal studies will be required to test this hypothesis.Acknowledgements
This work was supported by the National Institute of Diabetes and Digestive and Kidney Diseases (1R01DK097115-01A1) and by support in kind from Philips Healthcare. The authors are grateful for the contributions of Bertin Valdez, Thomas Hofstra, Jackie Baskim, Sue Carson, Trish Peterson and Debbie Harris for patient recruitment.References
1. Wood JC, Tyszka JM, Ghugre N, Carson S, Nelson MD, Coates TD. Myocardial iron loading in transfusion-dependent thalassemia and sickle-cell disease. Blood. 2004;103(5):1934-1936.
2. Wood JC, Cohen AR, Pressel SL, Aygun B, Imran H, Luchtman-Jones L, Thompson AA, Fuh B, Schultz WH, Davis BR, Ware RE. Organ iron accumulation in chronically transfused children with sickle cell anaemia: baseline results from the TWiTCH trial. Br J Haematol. 2016;172(1):122-130.
3. Wood JC. Cardiac iron across different transfusion-dependent diseases. Blood Rev. 2008;22 Suppl 2:S14-21.
4. Meloni A, Puliyel M, Pepe A, Berdoukas V, Coates TD, Wood JC. Cardiac iron overload in sickle-cell disease. Am J Hematol. 2014;89(7):678-683.
5. Noetzli LJ, Coates TD, Wood JC. Pancreatic iron loading in chronically transfused sickle cell disease is lower than in thalassaemia major. Br J Haematol. 2011;152(2):229-233.
6. Noetzli L, Coates T, Mittelman SD, Wood JC. Pancreatic iron and pancreatic function in Thalassemia. Blood. 2008;112:3876
7. Wood JC, Enriquez C, Ghugre N, Tyzka JM, Carson S, Nelson MD, Coates TD. MRI R2 and R2* mapping accurately estimates hepatic iron concentration in transfusion-dependent thalassemia and sickle cell disease patients. Blood. 2005;106(4):1460-1465.
8. Onishi Y, Hayashi T, Sato KK, Ogihara T, Kuzuya N, Anai M, Tsukuda K, Boyko EJ, Fujimoto WY, Kikuchi M. Fasting tests of insulin secretion and sensitivity predict future prediabetes in Japanese with normal glucose tolerance. J Diabetes Investig. 2010;1(5):191-195.
Figures