1658
Detection of Pancreatic Ductal Adenocarcinoma and Liver Metastases: Comparison of Contrast-enhanced MR Imaging with Ga-EOB-DTPA and Extracellular Contrast MaterialsYoshifumi Noda1, Satoshi Goshima1, Yukiko Takai1, Nobuyuki Kawai1, Hiroshi Kawada1, Yukichi Tanahashi1, Kimihiro Kajta1, and Masayuki Matsuo1
1Radiology, Gifu University, Gifu, Japan
Synopsis
Ga-EOB-DTPA-enhanced MR imaging is well established imaging modality for the detection of liver metastases. On the other hand, it is expected that the arterial enhancement of solid organs is weaker comparing with extracellular contrast materials (ECCMs) because of its lower dosage. Our results demonstrated that the signal intensity ratio of the pancreas, tumor-to-pancreas contrast-to-noise ratio, and diagnostic performance for detecting pancreatic ductal adenocarcinoma (PDAC) were comparable, but the sensitivity for detecting liver metastases was better in Ga-EOB-DTPA compared with ECCMs, which suggests the usefulness of Ga-EOB-DTPA for evaluating patients with PDAC.
Purpose
To compare the detectability of pancreatic ductal adenocarcinoma (PDAC) and liver metastases between contrast-enhcanced magnetic resonance (MR) imaging with gadolinium ethoxybenzyl diethylenetriamine pentaacetic acid (Ga-EOB-DTPA) and extracellular contrast materials (ECCMs).Materials and Methods
This retrospective study was approved by our institutional review board and written informed consent was waived. One hundred thirty-two patients (65 men and 67 women; mean 69.6 ± 9.6 years) with suspected of having a pancreatic disease based on either their clinical history or a previously performed computed tomography, underwent contrast-enhanced MR imaging with Ga-EOB-DTPA (EOB group; 72 patients) or with ECCMs (ECCM group: 60 patients). Sixty-five and eighteen PDACs were pathologically diagnosed in EOB and ECCM groups, respectively. The ECCMs included Gd-BT-DO3A (n = 28), Gd-DTPA (n = 27), and Gd-DOTA (n = 5). MR imaging was performed using a 1.5-T (Intera Achieva Nova Dual, Philips Healthcare) or 3-T MR system (Ingenia 3.0T CX, Philips Healthcare). The MR imaging protocols consisted of the following sequences: In-phase and opposed-phase T1-weighted axial gradient-recalled-echo imaging; breath holding three-dimensional fat-suppressed axial T1-weighted fast field-echo imaging; respiratory-triggered two-dimensional fat-suppressed axial T2-weighted turbo spin-echo imaging; and respiratory-triggered two-dimensional axial diffusion-weighted imaging with a single-shot echo-planar sequence. A dose of 0.1 mL/kg for Ga-EOB-DTPA and Gd-BT-DO3A, and 0.2 mL/kg for Gd-DTPA and Gd-DOTA was injected at a rate of 2 mL/sec followed by 30 mL saline flush at the same rate. The signal intensities of pancreatic parenchyma (SIpancreas), paraspinal muscle, and PDAC (SIPDAC) if present, were measured on the pre-contrast and arterial phase images. Background noise was quantified as the standard deviation (SD) of the signal intensity of the homogeneous region on the anterior abdominal wall fat tissue. The signal intensity ratio (SIR) of the pancreas was calculated as a ratio of signal intensity of the pancreatic parenchyma to that of paraspinal muscle. The tumor-to-pancreas contrast-to-noise ratio (CNR) was calculated the following equation: CNR = (SIpancreas – SIPDAC)/SD. The conspicuity of PDAC was evaluated on the arterial phase images, and that of liver metastases if present, was also evaluated on all MR images using a 5-point scale on a lesion-by-lesion base. The Mann-Whitney U and Fisher’s tests were conducted to evaluate differences in patients’ clinical data, SIR of the pancreas, CNR, sensitivity and specificity for the detection of PDAC, and sensitivity for the detection of liver metastases.Results
No significant differences were observed in patients’ age (P = 0.45), gender (P = 1.00), and maximum diameter of PDAC (P = 0.30). The SIR of the pancreas (P = 0.25) and CNR (P = 0.055) were comparable between EOB and ECCM groups (Figures 1 and 2). The sensitivity (93.8% vs 83.3%, P = 0.17) and specificity (100.0% vs 100.0%, P = 1.00) for the detection of PDAC were comparable between EOB and ECCM groups (Figures 3 and 4). Ninety-one and five liver metastases were confirmed in EOB and ECCM groups, respectively. EOB group had significantly greater sensitivity for the detection of liver metastases compared with ECCM group (95.6% vs 60.0%, P = 0.030).Discussion
In the present study, the SIR of the pancreas, CNR, and diagnostic performance for the detection of PDAC were comparable between EOB and ECCM groups. Other than the above, EOB group was significantly superior in detecting liver metastases compared with ECCM group. The ECCMs, including Gd-BT-DO3A, Gd-DTPA, and Gd-DOTA, have been used for more than two decades and well established. Recently, liver-specific contrast agent, Ga-EOB-DTPA have become available for the detection and characterization of focal liver lesions. The recommended dosage of Ga-EOB-DTPA is 0.025 mmol/kg, which is one-fourth of the recommended dosage of ECCMs. Therefore, it is expected that the arterial enhancement of solid organs is weaker comparing with ECCMs. In fact, a previous study reported that arterial enhancement of the pancreas was lower with Ga-EOB-DTPA compared with Gd-DTPA 1. They applied 3 mL/sec of injection rate as against 2 mL/sec of ours. By using a lower injection rate, the bolus is stretched, and has a greater chance to establish the protein binding process in human blood, which results in a higher relaxivity 2. Considering the detection of liver metastases, Ga-EOB-DTPA-enhanced MR imaging has excellent diagnostic performance, especially in lesions less than 10 mm in size 3. We believed that Ga-EOB-DTPA-enhanced MR imaging was all that is needed to examine pancreatic diseases because diagnostic performance for detecting PDAC were comparable and better in detecting liver metastases among the contrast materials. In conclusion, contrast-enhanced MR imaging with Ga-EOB-DTPA was equivalent to that with the other ECCMs in detecting PDAC and had better sensitivity in detecting liver metastases, which suggests the usefulness of Ga-EOB-DTPA for evaluating patients with PDAC.Acknowledgements
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.References
[1] Tamada T, Ito K, Sone T, et al. Dynamic contrast-enhanced magnetic resonance imaging of abdominal solid organ and major vessel: comparison of enhancement effect between Gd-EOB-DTPA and Gd-DTPA. J Magn Reson Imaging 2009;29(3):636-40. [2] Rohrer M, Bauer H, Mintorovitch J, Requardt M, Weinmann HJ. Comparison of magnetic properties of MRI contrast media solutions at different magnetic field strengths. Invest Radiol 2005;40(11):715-24. [3] Motosugi U, Ichikawa T, Morisaka H, et al. Detection of pancreatic carcinoma and liver metastases with gadoxetic acid-enhanced MR imaging: comparison with contrast-enhanced multi-detector row CT. Radiology 2011;260(2):446-53.Figures

Figure
1. Box
plot showing the
signal intensity ratio of the pancreas on arterial phase images. No significant
difference was found between EOB and ECCM
groups (P =
0.25).

Figure
2. Box
plot showing the
tumor-to-pancreas contrast-to-noise ratio.
No significant difference was found between EOB and ECCM groups (P =
0.055).
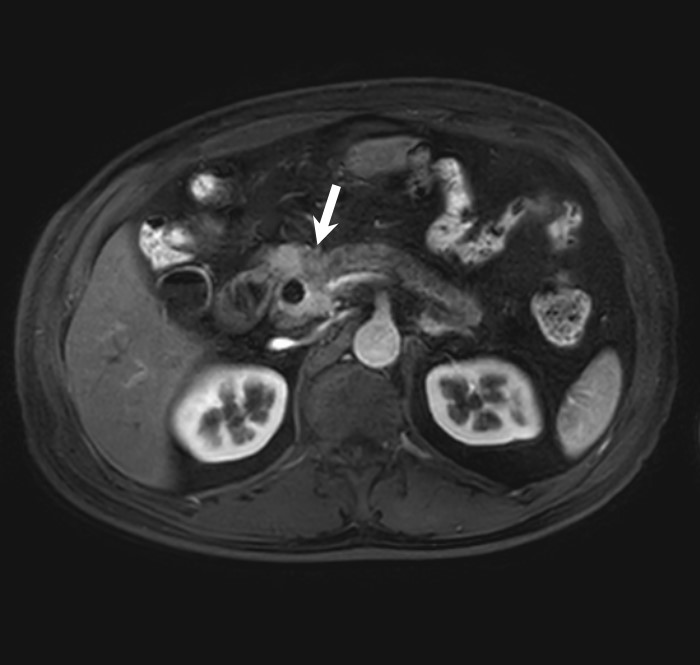
Figure
3.
Arterial
phase image in a 55-year-old man using
Ga-EOB-DTPA.
Pancreatic ductal adenocarcinoma in pancreatic head (arrow) is well visualized.

Figure
4.
Arterial
phase image in a 74-year-old man using
Gd-BT-DO3A. Pancreatic
ductal adenocarcinoma in pancreatic head (arrow) is also well visualized.