1653
Towards systematic evaluation of velocity-selective ASL in the measurement of placental perfusion1Department of Radiology, University Medical Center Utrecht, Utrecht, Netherlands, 2Center for Biomedical Engineering, King’s College London, London, United Kingdom, 3C.J. Gorter Center for high field MRI, Department of Radiology, Leiden University Medical Center, Leiden, Netherlands
Synopsis
The placenta’s role as a nutrient and oxygen source for the fetus highly depends on blood supply and thus perfusion may be a sensitive marker of placenta function. Velocity-selective arterial spin labeling (VSASL) placental perfusion measurements have previously been demonstrated using standard parameter settings from the brain. In this study, the influence of different VSASL parameter settings was assessed to optimize measurement of placental perfusion. The results of this study will improve our understanding and interpretation of the measured perfusion signals in the placenta.
Introduction
Placenta function plays an
important role in the development of the fetus during pregnancy. Blood supply
to the placenta, vascular abnormalities and the efficiency of oxygen transfer
from maternal to fetal blood are often related to placenta dysfunction,
therefore, perfusion may thus be a sensitive marker of placenta functioning.1
Arterial spin labeling (ASL) is a non-invasive method using magnetically labeled blood water as an endogenous tracer; this makes ASL attractive for placental applications, and early reports have begun to appear.2-6 Velocity-selective ASL (VSASL)7 seems to be well suited for placental perfusion measurements since flowing spins are tagged within a specific velocity range, also inside the imaging region, thereby reducing transit-time artifacts. However, up to now VSASL placental perfusion measurements have only been demonstrated using standard parameter settings from the brain.4,6 Therefore, we aimed to evaluate the influence of a number of VSASL parameter settings on the measurement of placental perfusion.
Methods
Eight volunteers in the second
trimester of pregnancy (gestational age (GA) median/range 29.5/24.0-33.7 weeks) with
anterior-located placentas, were included. A 3T Philips Achieva MR-scannerwas used, with a 32-channel cardiac coil. The
baseline imaging protocol was a VSASL 2D single-shot multi-slice FFE-EPI
sequence with background suppression (BGS): single-VS labeling module, post-labeling
delay (PLD) 1600 ms, cut-off velocity 1.6 cm/s, velocity-encoding direction anterior-posterior
(AP), field-of-view 350x350x52 mm3, acquired resolution (4 mm)3,
TR/TE 3500/20 ms, 13 coronal slices, maternal-to-fetal slice scan order, 26 label-control
pairs, acquisition time 3min16s. One label-control pair without BGS was added to
each scan (M0*) for normalization of the perfusion-weighted images. The
following VSASL parameter settings were evaluated: velocity-encoding direction
(AP, superior-inferior (SI), right-left (RL)), cut-off velocity (1, 2, 3.5, 7 cm/s),
PLD (400, 1000, 1600, 2200 ms), and number of VS labeling modules (single vs dual). A subset of parameter settings
was evaluated in each subject.
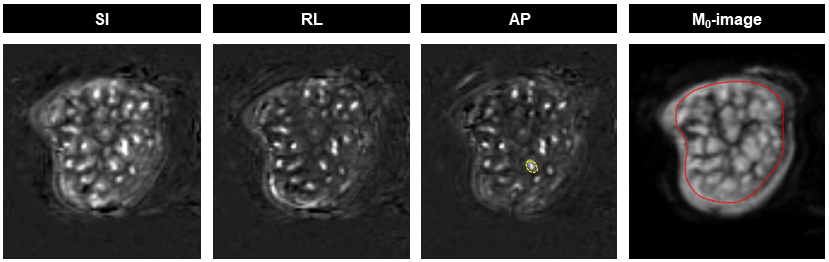
Post-processing included: non-rigid ANTs8 motion-correction within/between scans acquired in the same subject; pair-wise subtraction of the label-control pairs; averaging; division by M0* to yield averaged ΔM/M0 representing percent perfusion signal. Regions-of-interest (ROI) based analyses were performed in MeVisLab (MeVis Medical Solutions, Germany) to compare perfusion signal differences between different VSASL parameter settings. ROIs were drawn manually around the placenta on the M0* and around a focal region identified as hyperintense on ΔM/M0, putatively corresponding to localized placental units (Fig. 1).
Results and Discussion
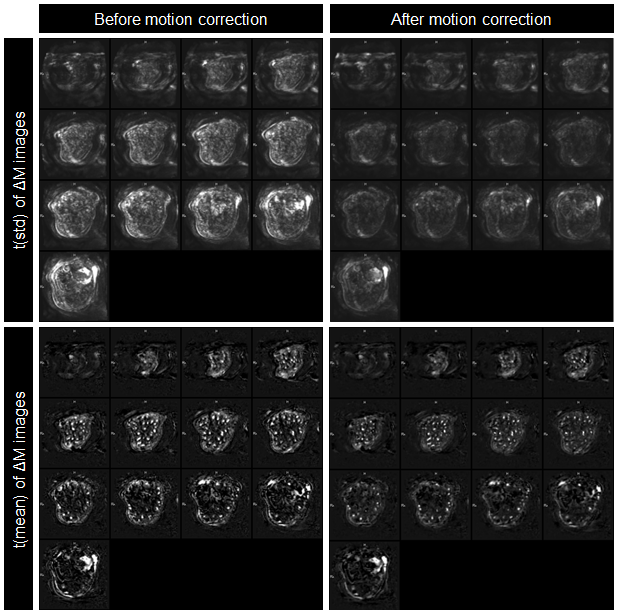
Images were analyzed for 6
subjects; 2 subjects were excluded due to poor image quality. Figure 2 demonstrates reduced
misalignment, measured as temporal standard deviation, after motion correction.
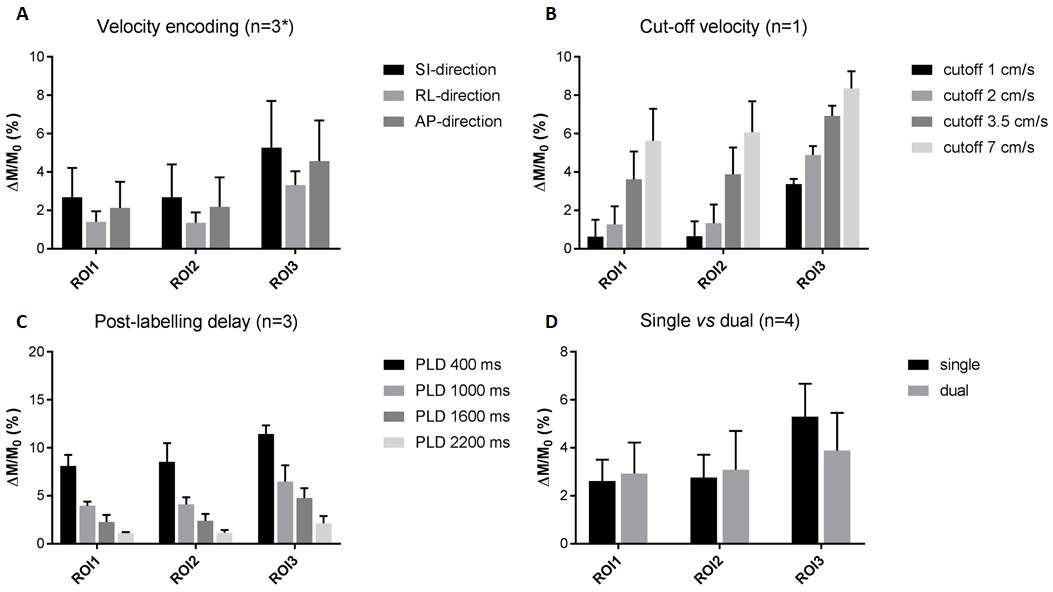
A summary of the ROI-based analyses for comparison of obtained perfusion signal
between the different parameter settings is shown in Figure 3.
Perfusion signal appeared highest
when encoding in AP- or SI-direction (Fig.
1, 3A). The arterial input
of the placenta can be multi-directional and the anatomical location of
the placenta can be variable. If these results are confirmed in further subjects and across GA, it might result beneficial to perform a combination
of velocity encoding directions in one acquisition (in an interleaved manner
for the acquired label-control pairs).
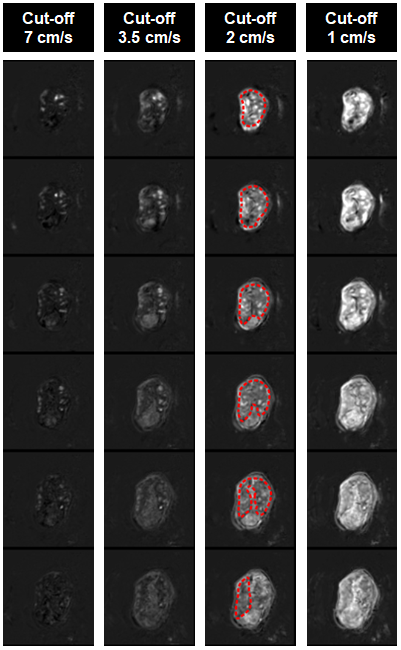
The perfusion signal decreased
with increasing cut-off velocity (Fig. 3B,
4). This preliminary observation (n=1) reflects the lower fraction of labeled blood with higher cut-offs. There
might be an interaction between blood velocity and labeling orientation that
we plan to further explore.
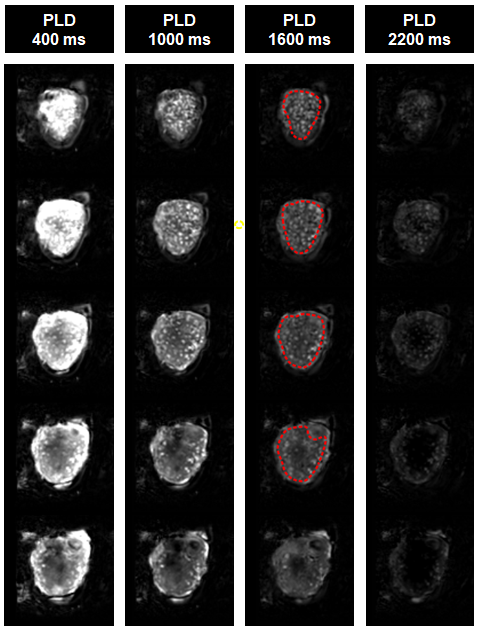
Observed perfusion decreased
with increasing PLD (Fig. 3C, 5) in
all subjects and ROIs. In contrast to brain ASL, within the PLD range analyzed, we did not observe any
placental region where the signal initially increases. Differences
in hematocrit and oxygenation level between maternal and fetal blood affect their
respective T1/T2 relaxation times9 and influence
their contribution to the apparent perfusion signal. Establishing the relative fraction of maternal to fetal blood observed requires further investigation.
Single and dual VS labeling modules appeared to give comparable perfusion signal in the whole placenta, but somewhat lower signal in focal hyperintense regions with dual VS labeling (Fig. 3D). This could be explained by increased T2-weighting due to the second labeling module in dual VS-labeling, or its suppression of blood accelerating during the PLD.
Conclusions and outlook
The current results indicate that the VSASL parameter settings do influence the measured perfusion signal in the placenta. With acquisitions on additional subjects, we will be able to confirm and strengthen the current results and optimize VSASL settings for placental perfusion measurements. Moreover, the combination of different settings gives greater insight into the complexity of placental circulation and improves our understanding and interpretation of perfusion signals measured in the placenta.Acknowledgements
We thank the midwives, obstetricians and radiographers who played a key role in obtaining the data sets. We would also like to thank all participating mothers. This work received funding from the NIH (Human Placenta Project - grant 1U01HD087202-01), the Wellcome Trust (Sir Henry Wellcome Fellowship, 201374/Z/16/Z), and the EPSRC (grants N018702 and M020533). This work was also supported by the Wellcome/EPSRC Centre for Medical Engineering [WT 203148/Z/16/Z]. This work is part of the research programme Drag and Drop ASL with project number NWO-TTW 14951, which is (partly) financed by the Netherlands Organisation for Scientific Research (NWO).References
1. Wigglesworth JS. Vascular anatomy of the human placenta and its significance for placental pathology. J Obstet Gynaec Brit Cwlth. 1969;76:979-989
2. Francis S, Duncan KR, Moor RJ, et al. Non-invasive mapping of placental perfusion. Lancet. 1998;351(9113):1397-9
3. Derwig I, Lythgoe DJ, Barker GJ, et al. Association of placental perfusion, as assessed by magnetic resonance imaging and uterine artery Doppler ultrasound, and its relationship to pregnancy outcome. Placenta. 2013;34:885-891
4. Zun Z, Zaharchuk G, Andescavage NN, et al. Non-Invasive Placental Perfusion Imaging in Pregnancies Complicated by Fetal Heart Disease Using Velocity-Selective Arterial Spin Labeled MRI. Sci Rep. 2017;7(1):16126
5. Shao X, Liu D, Martin T, et al. Measuring human placental blood flow with multidelay 3D GRASE pseudocontinuous arterial spin labeling at 3T. J Magn Reson Imaging. 2018;47(6):1667-1676
6. Zun Z, Limperopoulus C. Placental perfusion imaging using velocity-selective arterial spin labeling. Magn Reson Med. 2018;80(3):1036-1047
7. Wong EC, Cronin M, Wu WC, et al. Velocity-selective arterial spin labeling. Magn Reson Med. 2006;55(6):1334-41
8. Avants B, Epstein C, Grossman M, et al. Symmetric diffeomorphic imageregistration with cross-correlation: Evaluating automated labeling of elderly and neurodegenerative brain. Medical Image Analysis. 2008;12(1):26-41
9. Liu P, Chalak LF, Krishnamurthy LC, et al. T1 and T2 values of human neonatal blood at 3 Tesla: Dependence on hematocrit, oxygenation, and temperature. Magn Reson Med. 2016;75(4):1730-5
Figures