1645
Pseudo continuous arterial spin labeling perfusion MRI of advanced rectal cancer: utility in predicting response to neoadjuvant chemotherapy1Kagoshima University, Kagoshima, Japan, 2Philips Electronics, Japan, Tokyo, Japan
Synopsis
This study focused on the feasibility of pseudo
continuous arterial spin labeling (pCASL) perfusion MRI as a tool for
predicting the response of advanced rectal cancer treated with neoadjuvant
chemotherapy. Correlation
between reduction rate of rectal cancer after chemotherapy and blood flow (BF)
derived from pCASL or DCE MRI parameters within tumors was evaluated. Our results showed significant positive
correlations between tumor reduction rate and BF (p = 0.001, ρ = 0.644) or Ktrans
(p = 0.003, ρ= 0.579). These results suggested pCASL may have the
potential to predict the treatment response of neoadjuvant chemothoerpy for
advanced rectal cancer.
Introduction
Neoadjuvant therapy followed by total mesorectal excision is the standard treatment for locally advanced rectal cancer. Pharmacokinetic parameters of dynamic contrast-enhanced MRI (DCE-MRI) such as Ktrans (forward volume transfer constant), Kep (reverse reflux rate constant between extracellular space and plasma) and Ve (the fractional volume of extracellular extravascular space per unit volume of tissue) are relevant as they are known to correlate with neoangiogenesis, that leads to immature and unstable vessels with increased leakiness, and are important factors with regard to response prediction and evaluation after chemoradiotherapy for locally advanced rectal cancer. Pseudo continuous arterial spin labeling (pCASL) perfusion MRI is a noninvasive, nonradioactive and non-contrast-enhanced method capable of quantitatively measuring microvascular perfusion characteristics of tissues. However, the usefulness of pCASL for assessing the therapeutic response to neoadjuvant chemotherapy (NAC) for advanced rectal cancer has not been elucidated. Therefore, the objective of this study was to evaluate the usefulness of pCASL for predicting the therapeutic response to NAC for advanced rectal cancer in comparison with perfusion parameters derived from DCE MRI.Methods
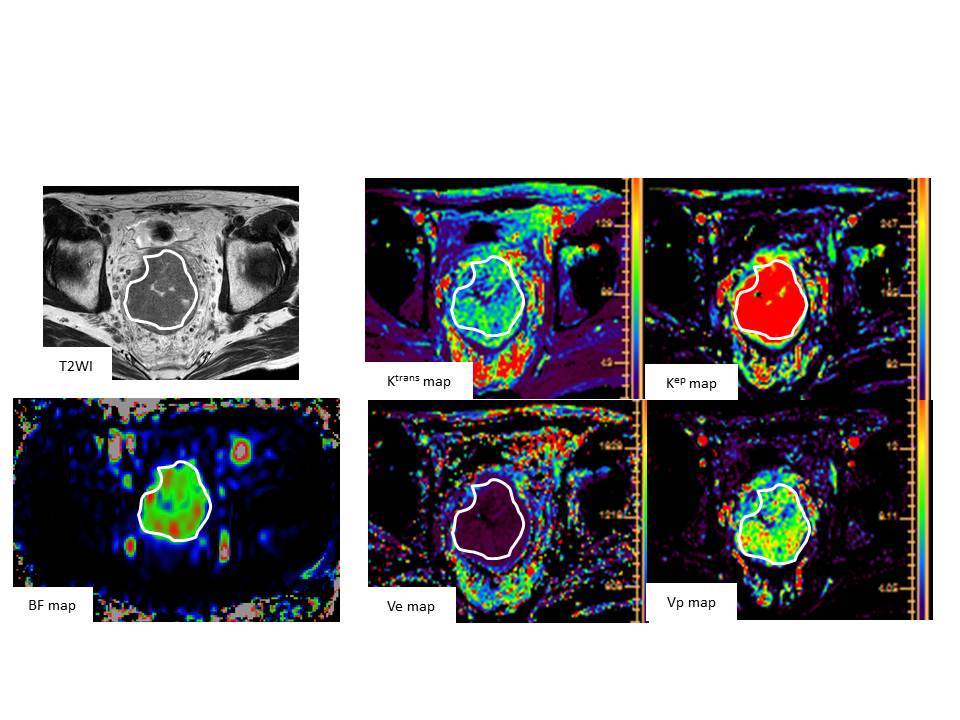
Our study population consisted of 24 patients (16 men, 8 women; mean age, 64 years; range, 26–75 years) with histologically confirmed rectal cancer underwent 3D-pCASL and DCE MRI. The pCASL MRI was acquired by 3D VISTA using a 3T MRI. The labeling plane was 80 mm above the center of the image FOV. Labeling was applied for 3 sec followed by a 1.6-sec post labeling delay before image acquisition. The total scan time of pCASL examination was 4 min 7 sec. Others pCASL parameters were as follows: TR/TE = 6500/36 ms, slice thickness = 5.0 mm, FOV = 230×230 mm, matrix = 192×192. For the DCE-MRI study, a bolus of gadolinium-DTPA (0.1mmoL/kg) was injected into a vein at an injection rate of 3.0 mL/sec using an automated injector and was followed by a 25-mL saline flush. The temporal resolution of 3D-FFE sequence was approximately 3.4 sec, and dynamic data acquisition was started after the contrast medium injection and repeated 95 times. For T1 maps, precontrast 3D-FFE with dual flip angles (5o and 15o) was performed. We analyzed the association between reduction rate of rectal cancer at 6 months after chemotherapy and blood flow (BF) derived from pCASL or DCE MRI parameters, such as Ktrans, Kep, Ve and Vp (vascular plasma volume) within tumors (Figure1). Spearman’s bivariate correlation was used to assess the relationship between the tumor reduction rate and BF or DCE MRI-derived parameters.Results
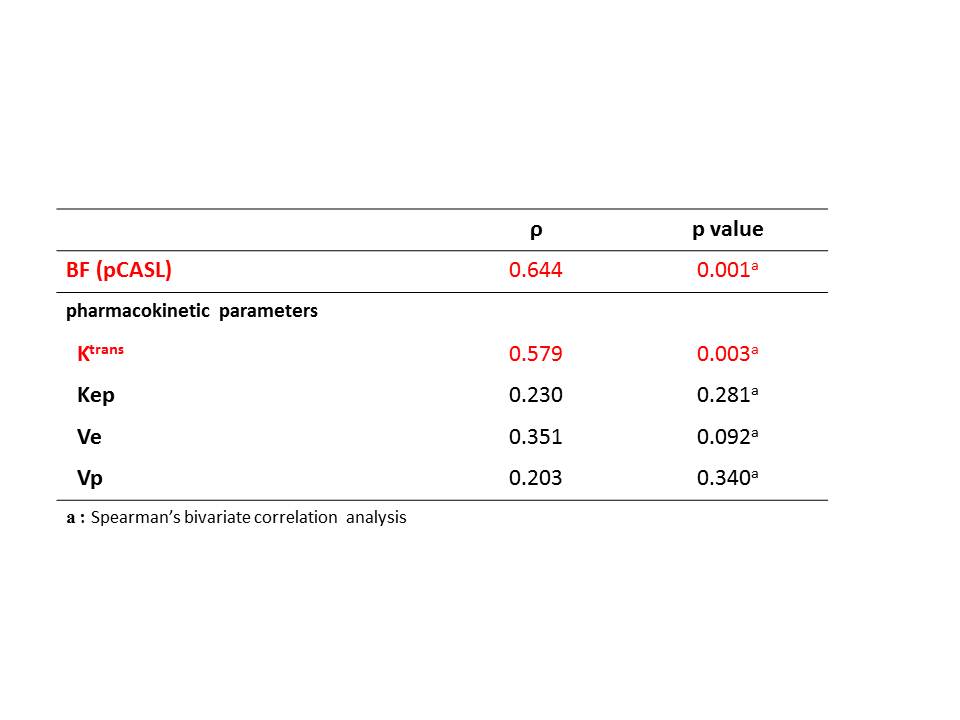
There were significant positive correlations between tumor reduction rate and BF (p = 0.001, r = 0.644) or Ktrans (p = 0.003, ρ= 0.579) (Figure 2). No significant correlation with tumor reduction rate was shown in Kep (p = 0.281), Ve (p = 0.092) or Vp (p = 0.340).Discussion
In this study, there were significant positive correlations between tumor reduction rate and BF or Ktrans. Several studies have shown that Ktrans is the most important pharmacokinetic parameter of DCE MRI with regard to predict the tumor response after chemoradiotherapy (CRT) for rectal cancer 1,2. A high Ktrans indicates high permeability and vascularity of the tumor, which is believed to make the tumor more accessible to CRT2,3. No previous studies have shown the usefulness of pCASL for predicting tumor response after chemotherapy or CRT. Our results suggested that BF derived from pCASL could be useful for response prediction after chemotherapy for advanced rectal cancer alternative to DCE MRI.Conclusion
pCASL may have the potential to predict the treatment response of neoadjuvant chemotherapy for advanced rectal cancer.Acknowledgements
No acknowledgement found.References
1. Lim JS, Kim D, Baek S, et al. Perfusion MRI for the prediction of treatment response after preoperative chemoradiotherapy in locally advanced rectal cancer. Eur Radiol 2012; 22:1693-1700
2. Tong T, Sun Y, Golub M, et al. Dynamic contrast-enhanced MRI: Use in predicting pathological complete response to neoadjuvant chemoradiation in locally advanced rectal cancer. Magn Reson Imaging 2015; 42:673-680
3.
Yeo D, Oh S, Jung C, et al. Correlation of dynamic
contrast-enhanced MRI perfusion parameters with angiogenesis and bilologic
aggressiveness of rectal cancer: preliminary results. Magn Reson Imaging 2015;
41:474-480
Figures