1642
Dynamic contrast-enhanced MRI of the liver: comparison between radial VIBE with k-space weighted image contrast reconstruction (r-VIBE-KWIC) and Golden-angle RAdial Sparse Parallel (GRASP)Yasunari Fujinaga1, Akira Yamada1, Ayumi Ohya1, Hirokazu Tokoro1, Takeshi Suzuki1, Hayato Hayashihara2, Aya Shiobara2, Yasuo Adachi2, Yoshihiro Kitou2, Marcel Dominik Nickel3, Terumasa Takemaru4, Hirokazu Kawaguchi5, and Katsuya Maruyama5
1Department of Radiology, Shinshu University, School of Medicine, Matsumoto, Japan, 2Radiology Division, Shinshu University Hospital, Matsumoto, Japan, 3MR Application Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 4Department of Application, Siemens Healthcare K. K., Tokyo, Japan, 5Diagnostic Imaging Business Area, DI Research & Collaboration Dpt., Siemens Healthcare K. K., Tokyo, Japan
Synopsis
We aimed to evaluate the differences of the DCE-MR images between radial VIBE with k-space weighted image contrast reconstruction (r-VIBE-KWIC) and Golden-angle RAdial Sparse Parallel (GRASP). DCE-MRI using r-VIBE-KWIC and GRASP was performed in 36 and 35 patients, respectively. The most optimal arterial phase image was selected from eight sub-frame images at arterial phase, and factors of image quality in the both two groups were assessed using five-point scales. In GRASP, the median scores for all factors except for one were significantly higher than those in r-VIBE-KWIC. In conclusion, GRASP provided the better DCE-MR images than r-VIBE-KWIC.
INTRODUCTION
High-spatial and -temporal resolution dynamic contrast-enhanced MRI (DCE-MRI) of the liver using the radial volumetric interpolated breath-hold examination with k-space weighted image contrast reconstruction (r-VIBE-KWIC) has advantages such as optimal scan timing, less motion artifact, detailed hemodynamic evaluation of lesions1,2. Recently, compressed sensing Golden-angle RAdial Sparse Parallel (GRASP), which is a golden-angle radial acquisition combined with compressed sensing reconstruction technique, has been available for DCE-MRI of the liver3,4. In this study, we aimed to evaluate the differences of the DCE-MR images between r-VIBE-KWIC and GRASP.MATERIALS AND METHODS
This study was a prospective observation study, and the study design was approved our institutional review board. Written informed consent was obtained from all participating patients before MRI examinations. Consecutive seventy-one patients who underwent breath-holding dynamic contrast-enhanced MRI (DCE-MRI) of the liver at two kinds of 3-tesla MR units were enrolled in this study. Thirty-six patients (24 men and 12 women; mean age 65.6 years old) were performed DCE-MRI using r-VIBE-KWIC between January 2018 and march 2018 (r-VIBE-KWIC group). Thirty-five patients (21 men and 14 women; mean age 64.3 years old) were performed DCE-MRI using GRASP between April 2018 and July 2018 (GRASP group). Scan parameters of the two sequences were shown in table 1. Standard dose of Gd-EOB-DTPA (0.025 mmol/kg body weight) were used in all patients. The contrast agent was injected from the cubital vein at the rate of 2 mL/s followed by 50 mL of 0.9% saline at the same rate. Arterial phase images were obtained 22 s after the injection started. Of the eight sub-frame of the arterial phase images, the most optimal arterial phase image was selected and factors of image quality were assessed using five-point scales as follows: visualization of the right and left hepatic arteries (5, excellent, diagnostic; 4, good, diagnostic; 3, fair, diagnostic; 2, poor, non-diagnostic; 1, non-detectable, non-diagnostic), degree of the artifact at right lobe, left lobe and caudate lobe based on the visualization of intrahepatic vessels and the homogeneity of the hepatic parenchyma (5, no artifact, diagnostic; 4, faint, diagnostic; 3, moderate, diagnostic; 2, intermediate, non-diagnostic; 1, strong, non-diagnostic), and overall image quality (5, excellent, diagnostic; 4, good, diagnostic; 3, fair, diagnostic; 2, poor, non-diagnostic; 1, very poor, non-diagnostic). The scores of the two groups were compared using Mann-Whitney U test. In each group, the score of each lobe was compared using Kruskal-Wallis test and Dunn’s multiple comparison test.RESULTS
The median scores of overall, right hepatic artery, left hepatic artery, artifact at right lobe, left lobe and caudate lobe in r-VIBE-KWIC/GRASP were 3/4, 2/4, 2/4, 3/4, 3.5/4 and 3/3, respectively. For all factors except for artifact at caudate lobe, the scores in the GRASP group were significantly higher than those in r-VIBE-KWIC group (Figure 1, 2). Regarding artifact, the score for the caudate was significantly lower than other groups in each group (Figure 3). A representative case was shown in Figure 4.DISCUSSION
There is no report analyzing image quality of breath-holding DCE-MRI using GRASP because GRASP has been used for free-breathing DCE-MRI. In this sense, optimization of the breath-holding GRASP was challenging. Regarding GRASP, number of spokes used for one sub-frame images was 21. In this study, hepatic arteries were clearly seen in GRASP than in r-VIBE-KWIC. Because the acceleration factor was 21.5, the sub-frame image had the image quality equivalent to the image with 451.5 (21 x 21.5) spokes, that was more than r-VIBE-KWIC (198–208 spokes). In addition, GRASP allowed smaller the voxel size (about 5.5 mm3) than that of r-VIBE-KWIC (about 15.3 mm3) even though breath-holding time was similar in both r-VIBE-KWIC and GRASP. The advantage of the GRASP in the parameter setting might be the reason for the better visualization of the hepatic arteries. This result may indicate GRASP has a potential to demonstrate detailed structures of the normal anatomy and the lesions. Artifact in GRASP was equal or weaker than that in r-VIBE-KWIC. We attributed the reason to artifact reduction by iterative reconstruction. However, artifact at the caudate lobe was worse than that at other lobes in both r-VIBE-KWIC and GRASP. The reason was unclear but it may be a disadvantage of radial sequences.CONCLUSION
Better visualization of the hepatic arteries and less artifact of the hepatic parenchyma were provided in GRASP than in r-VIBE-KWIC.Acknowledgements
No acknowledgement found.References
- Fujinaga Y, Ohya A, Tokoro H, Yamada A, Ueda K, Ueda H, et al. Radial volumetric imaging breath-hold examination (VIBE) with k-space weighted image contrast (KWIC) for dynamic gadoxetic acid (Gd-EOB-DTPA)-enhanced MRI of the liver: advantages over Cartesian VIBE in the arterial phase. Eur Radiol. 2014;24(6):1290-9.
- Kurozumi M, Fujinaga Y, Kitou Y, Yamada A, Ohya A, Adachi Y, et al. Evaluation of hemodynamic imaging findings of hypervascular hepatocellular carcinoma: comparison between dynamic contrast-enhanced magnetic resonance imaging using radial volumetric imaging breath-hold examination with k-space-weighted image contrast reconstruction and dynamic computed tomography during hepatic arteriography. Jpn J Radiol. 2018;36(4):295-302.
- Chandarana H, Feng L, Ream J, Wang A, Babb JS, Block KT, et al. Respiratory Motion-Resolved Compressed Sensing Reconstruction of Free-Breathing Radial Acquisition for Dynamic Liver Magnetic Resonance Imaging. Invest Radiol. 2015;50(11):749-56.
- Feng L, Axel L, Chandarana H, Block KT, Sodickson DK, Otazo R. XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magn Reson Med. 2016;75(2):775-88.
Figures
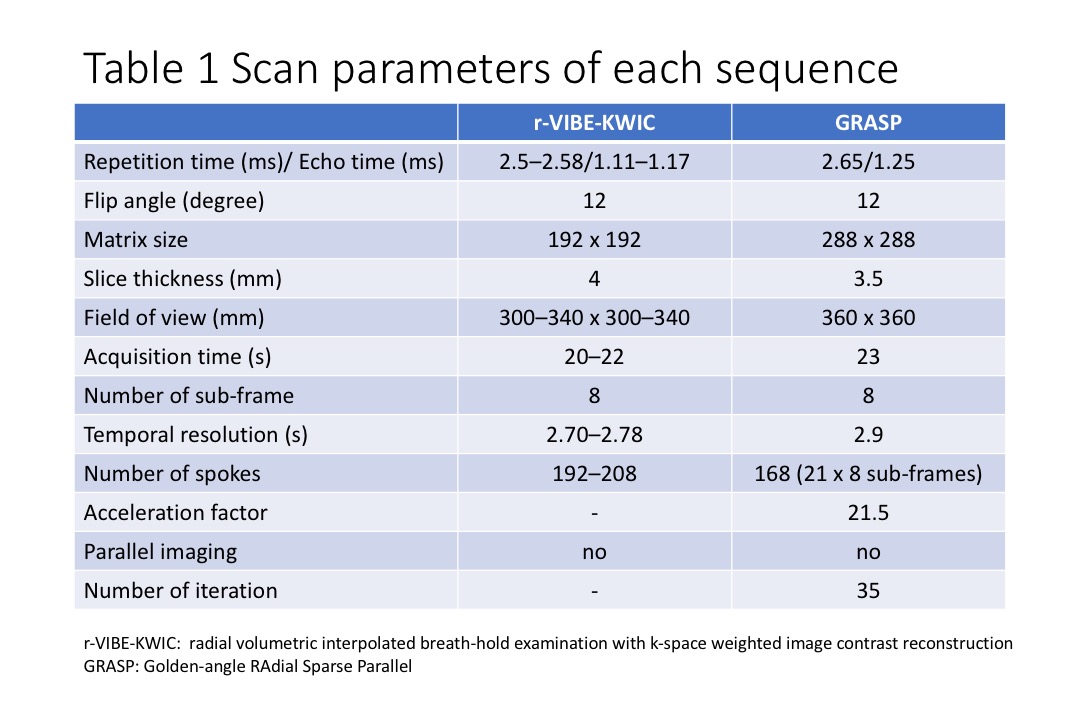
Table 1. Scan parameters of each sequence
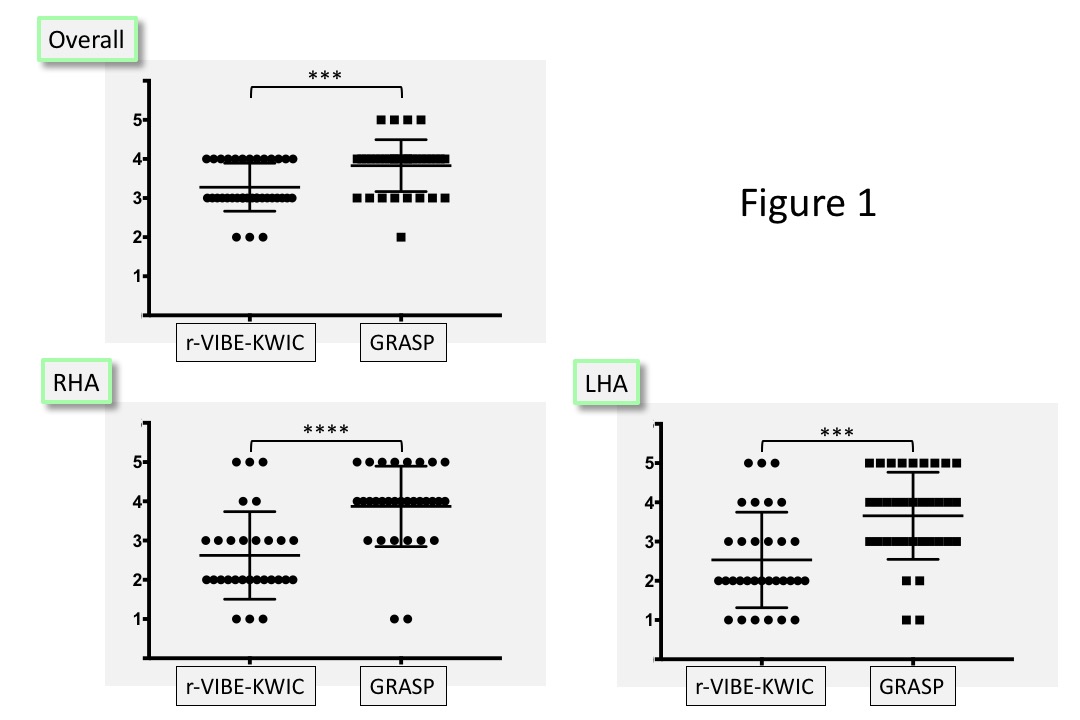
Figure 1. The score for
overall, right hepatic artery and left hepatic artery. ***, P < 0.001;
****, P < 0.0001
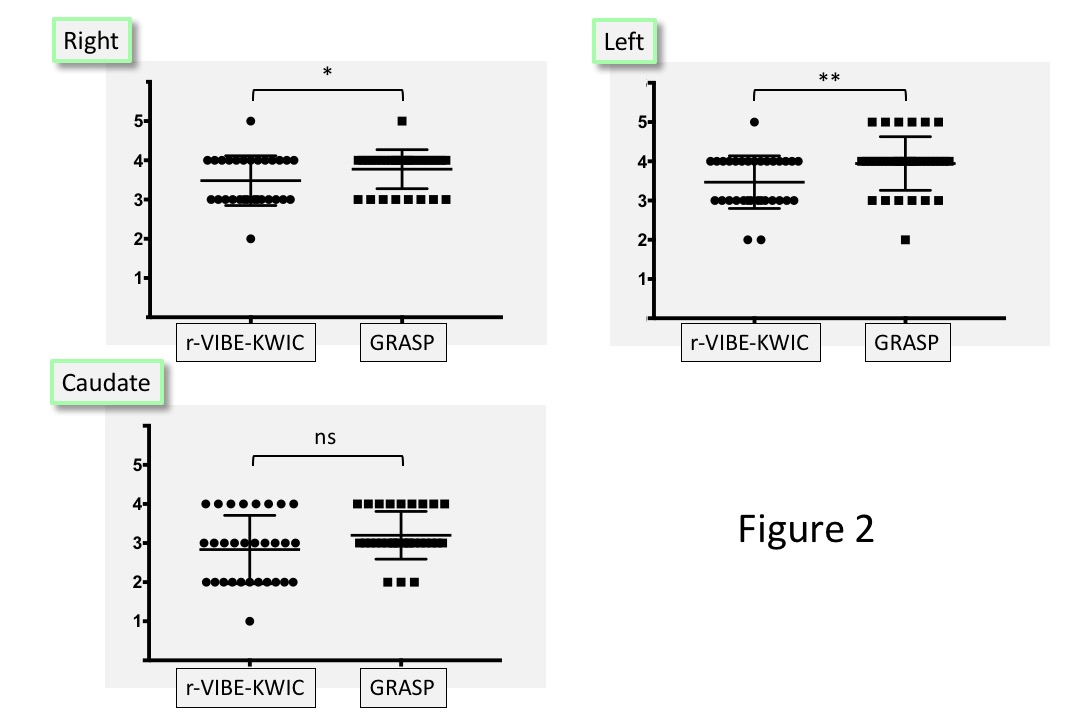
Figure 2. The score for
degree of the artifact at right, left and caudate lobe. *, P < 0.05; **, P
< 0.01
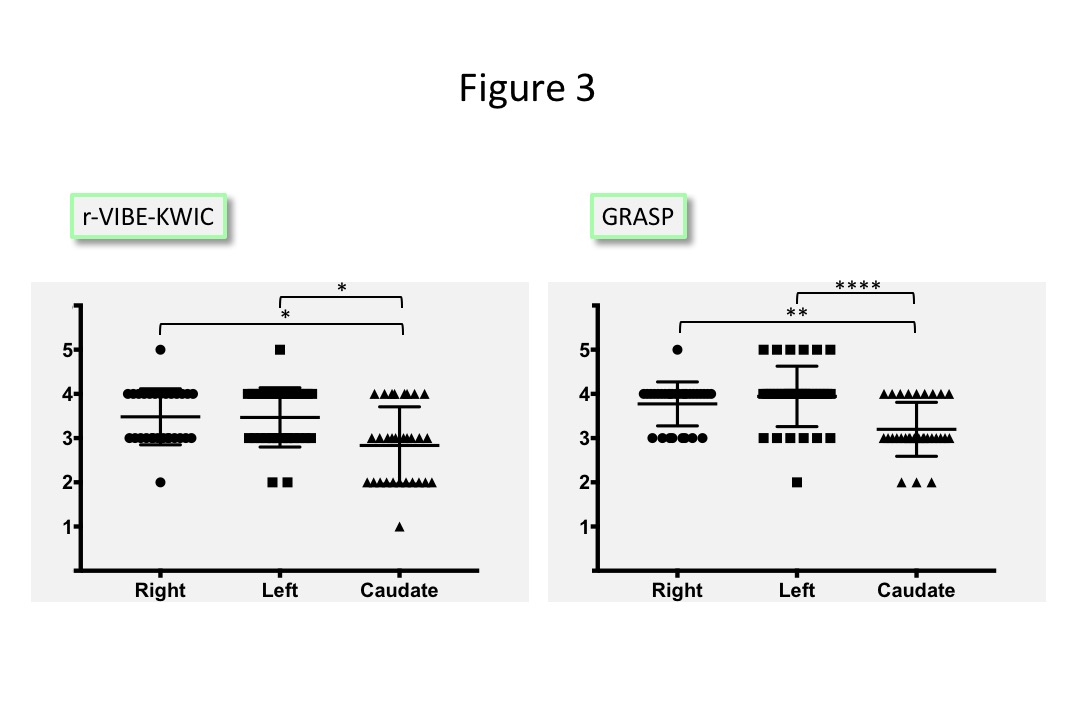
Figure 3. Comparison of the artifact between the
lobe. *, P , 0.05; **, P < 0.01; ****, P
< 0.0001
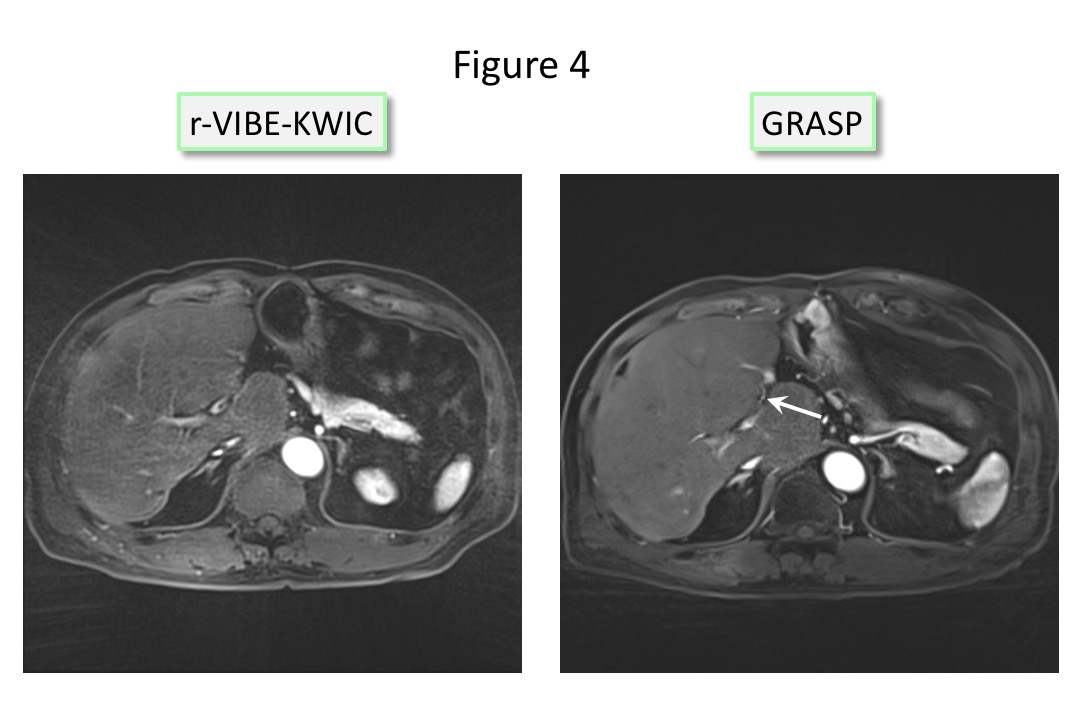
Figure 4. Arterial phase images of r-VIBE-KWIC and
GRASP. Left
hepatic artery in GRASP
(arrow) is clearly visible compared with that in r-VIBE-KWIC, and artifact at the right
lobe of the liver in GRASP is weaker than that in r-VIBE-KWIC.