1637
Motion robust two-minute free-breathing hepatobiliary phase imaging of the liver using a golden-angle ordered conical acquisition with extended readout.1Department of Radiology, Stanford University, Palo Alto, CA, United States, 2Electrical Engineering, Stanford Univresity, Palo Alto, CA, United States
Synopsis
Imaging of the liver can be compromised by motion artifacts which are especially problematic in patients with breathing difficulties. Non-Cartesian k-space sampling trajectories are motion robust and have shown promise in hepatobiliary-phase (HBP) imaging of the liver. Here we demonstrate that free-breathing HBP imaging can be obtained using a 3D cones k-space trajectory with golden angle ordering and extended readout (T1gER). The protocol shows similar performance to a conventional respiratory navigated sequence and can be acquired in less than half the time.
Introduction
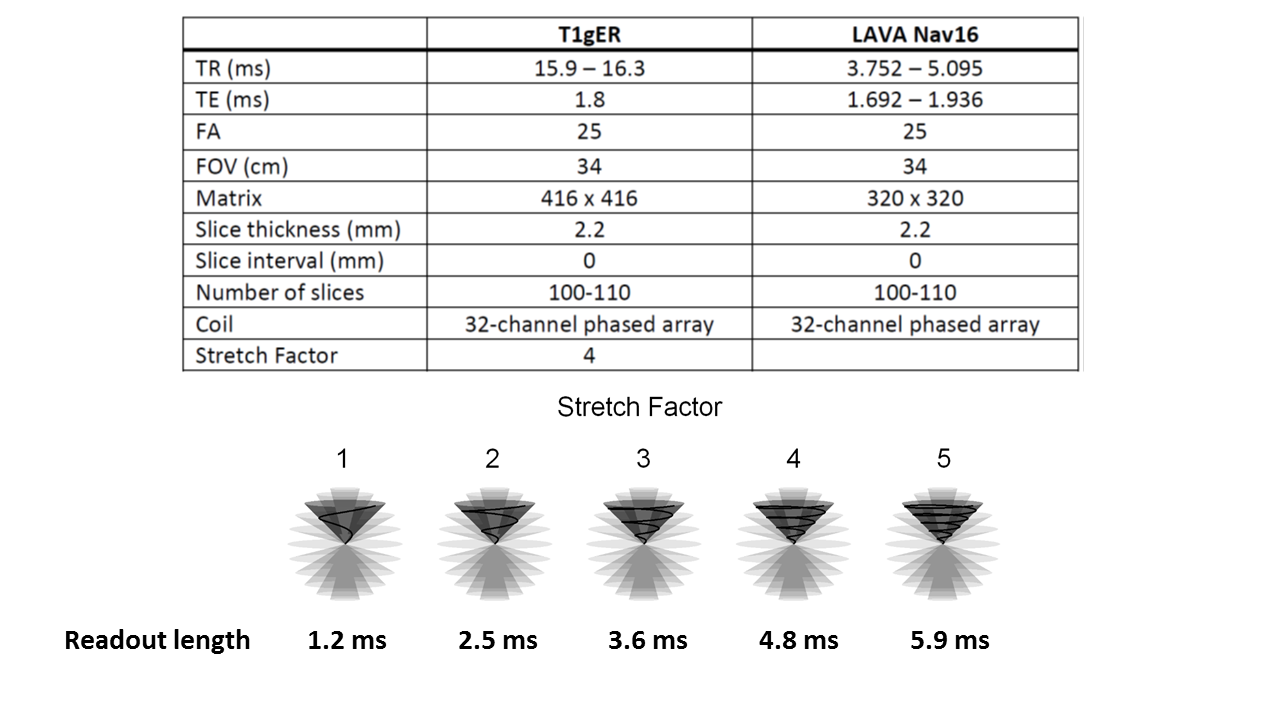
Hepatobiliary-phase (HBP) magnetic resonance imaging (MRI) of the liver has been valuable in lesion characterization and preoperative assessment of anatomy 1. Navigated or breath-hold sequences are generally used to minimize the effects of motion, which can drastically reduce image quality in the upper abdomen. This poses a problem in the subset of patients who cannot hold their breath or have difficulty following breathing instructions. Non-Cartesian k-space trajectories are motion robust 2, and several studies have demonstrated promising results using radial 3-5 or stack of spiral 6-8 trajectories for imaging of the liver. Although radial trajectories are fully non-Cartesian in three dimensions, they have low sampling efficiency. Conversely, stack of spiral trajectories have high sampling efficiency but may have coherent ghosting in the slice direction, which remains Cartesian. Here we assess the feasibility of free-breathing HBP imaging of the liver using a 3D cones k-space trajectory with golden angle ordering 9 to obtain true 3D non-Cartesian imaging with high sampling efficiency. Similar to spiral imaging and EPI, cones k-space sampling offers the ability to control and improve scan efficiency by prescribing how much data to collect per TR in what we call extended readout (Figure 1). We also compare its performance with that of a conventional respiratory navigated 3D gradient-echo sequence. The protocol presented here includes an extended readout to reduce scan time, with retrospective application of a soft-gating algorithm 10.Methods
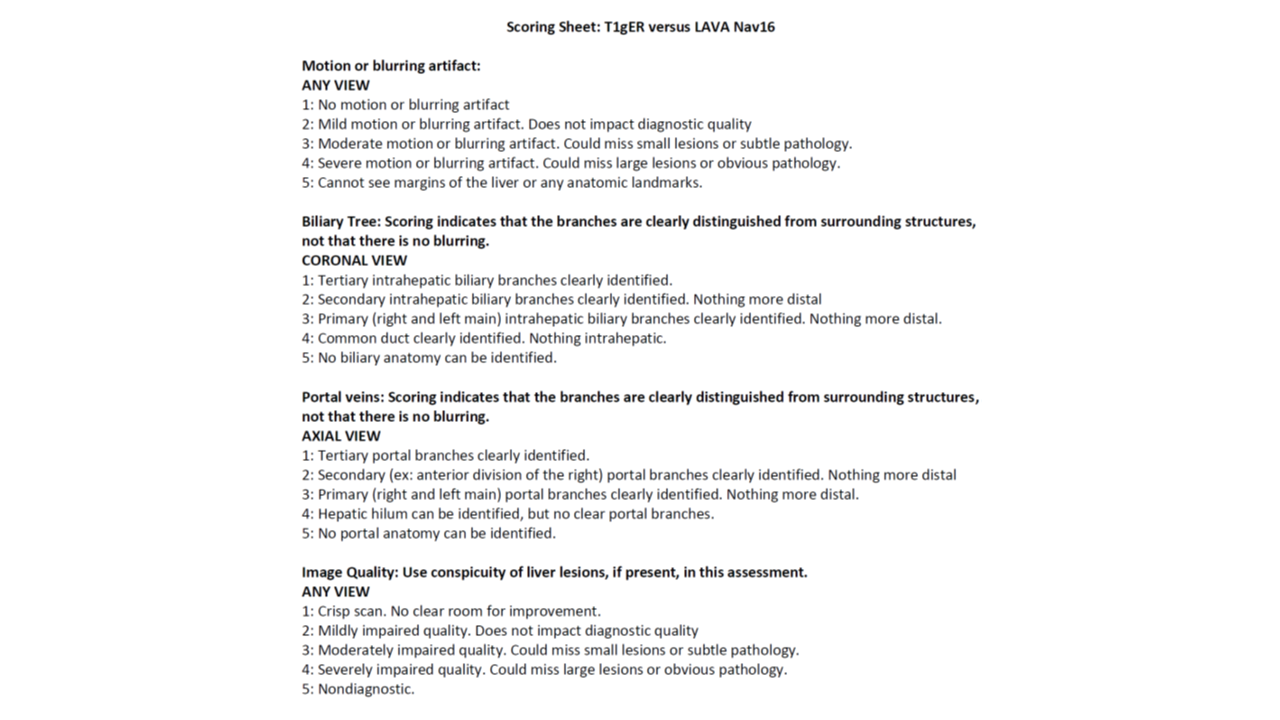
This retrospective study was conducted with institutional review board approval and informed consent waiver. Twenty consecutive patients undergoing Gadoxetate-enhanced MRI on one of six 3T scanners (GE MR 750, GE Healthcare, Waukeshaw WI) located at four different outpatient facilities were identified. Patient demographics were extracted from the electronic medical record. Complete image sets from both the T1-weighted SPGR sequence with cones trajectory and golden angle ordering with extended readout (T1gER) and the 16-minute navigated LAVA sequence (Nav16) were anonymized and randomized. Two radiologists independently scored the images for motion artifact, biliary tree visibility, portal vein visibility, and overall image quality using a 5-point scale (Figure 2). Wilcoxon rank-sum test was used to assess for equivalence between T1gER and Nav16 imaging, with p < 0.05 considered significant. Interobserver agreement was assessed using the intraclass correlation coefficients (ICC).Results
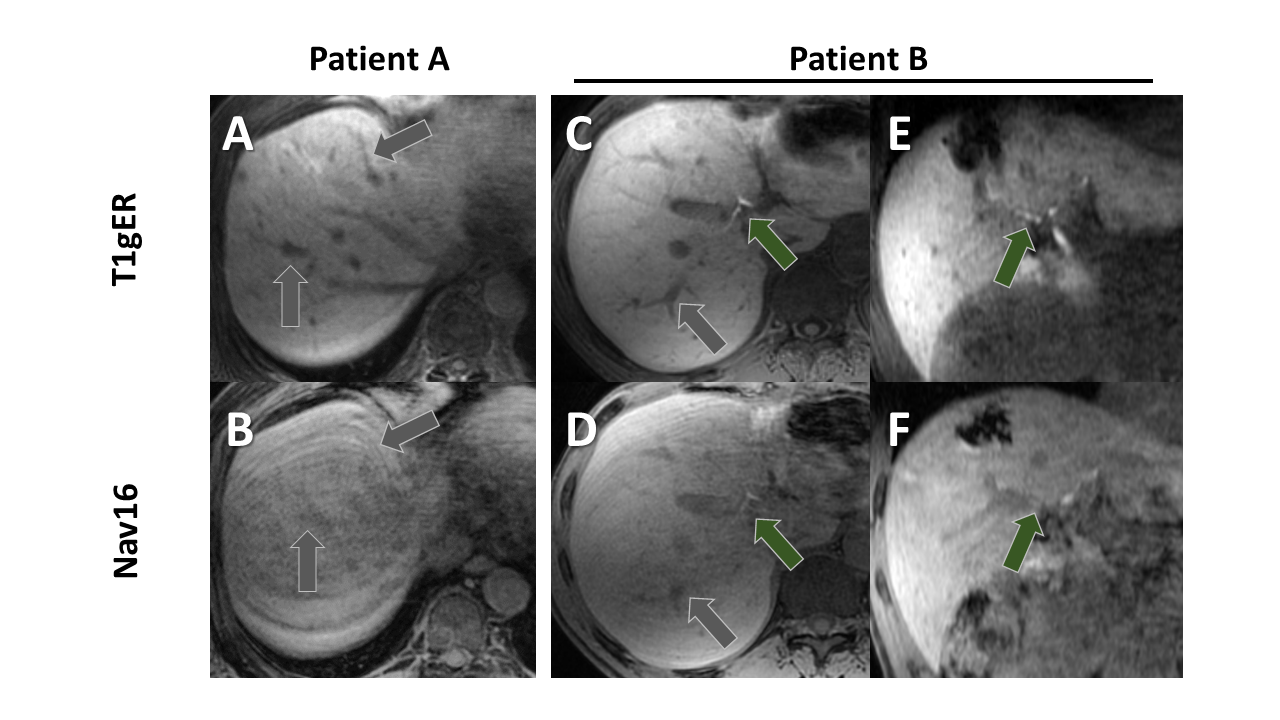
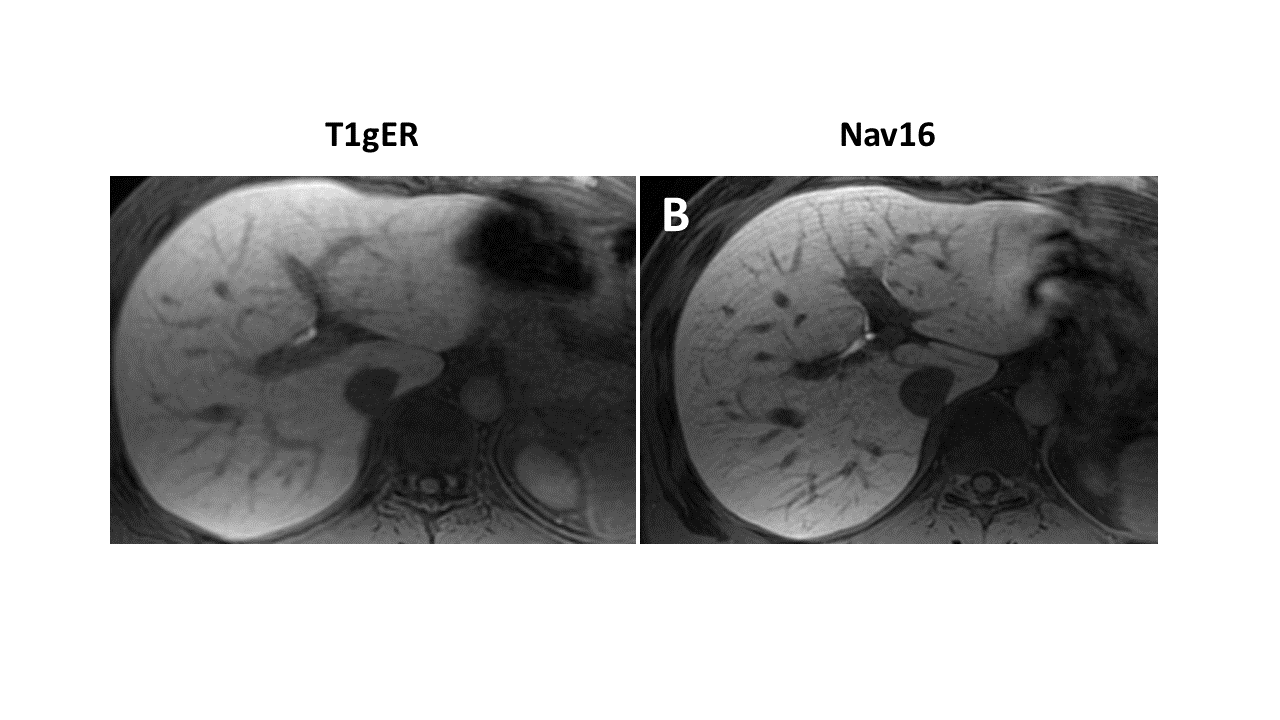
The 20 patients were 45% female (9/20) with a mean age of 53 (range 23-72) and mean BMI of 27.5 (range 19.4-39.4). Study indications included metastatic workup (80%; 16/20) and lesion evaluation (20%; 4/20). The T1gER acquisition took an estimated 2 minutes and 10 seconds while the navigated sequence acquisition took an estimated average time of 5 minutes. There was no significant difference in motion artifact (p=0.72/0.27, Reader A/B), delineation of the biliary tree (p=0.15/0.41), delineation of the portal veins (p=0.30/0.82), or overall image quality (p=0.60/0.46) between the two techniques, noting the average scores for Nav16 tended to be slightly better. Reader A and B both rated T1gER superior to Nav16 in several patients (Figure 3). Interobserver agreement was excellent in the assessment of T1gER motion artifact (ICC = 0.83, 95% CI 0.57-0.93) and overall image quality (ICC = 0.83, 95% CI 0.56-0.93). There was moderate agreement in the assessment of the biliary tree (ICC = 0.67) and portal veins (ICC = 0.64).Discussion
Here we demonstrate that high quality free breathing HBP imaging can be acquired in approximately 2 minutes using a 3D conical sampling trajectory and extended readout, offering similar overall performance to navigated GRE sequences with shorter acquisition time and without the need for respiratory navigation. Additionally, T1gER was able to outperform the navigated sequence in a subset of patients. This small study included only a few patients with breathing difficulties, and there was no formal assessment of imaging performance in this target population. A future study will be needed to more carefully evaluate the utility of T1gER in this subset of patients. We also noted some challenges with susceptibility artifact in the T1gER sequence which is exacerbated with extended readouts, thus future efforts will be aimed to optimizing the balance between reduced scan time and tolerance to field inhomogeneities.Conclusion
T1gER may offer a new tool for acquiring high quality HBP imaging in patients with breathing difficulties or challenges following breathing instructions and can reduce on-scanner time over navigated sequences.Acknowledgements
Grant support of NIH R01EB009690, R01 EB026136, R01HL136965, and GE Healthcare.References
1. Goodwin, M. D., Dobson, J. E., Sirlin, C. B., Lim, B. G. & Stella, D. L. Diagnostic challenges and pitfalls in MR imaging with hepatocyte-specific contrast agents. Radiographics 31, 1547-1568, doi:10.1148/rg.316115528 (2011).
2. Zucker, E. J., Cheng, J. Y., Haldipur, A., Carl, M. & Vasanawala, S. S. Free-breathing pediatric chest MRI: Performance of self-navigated golden-angle ordered conical ultrashort echo time acquisition. J Magn Reson Imaging 47, 200-209, doi:10.1002/jmri.25776 (2018).
3. Chandarana, H. et al. Free-breathing radial 3D fat-suppressed T1-weighted gradient echo sequence: a viable alternative for contrast-enhanced liver imaging in patients unable to suspend respiration. Invest Radiol 46, 648-653, doi:10.1097/RLI.0b013e31821eea45 (2011).
4. Budjan, J. et al. Rapid Cartesian versus radial acquisition: comparison of two sequences for hepatobiliary phase MRI at 3 tesla in patients with impaired breath-hold capabilities. BMC Med Imaging 17, 32, doi:10.1186/s12880-017-0203-y (2017).
5. Hedderich, D. M. et al. Clinical Evaluation of Free-Breathing Contrast-Enhanced T1w MRI of the Liver using Pseudo Golden Angle Radial k-Space Sampling. Rofo 190, 601-609, doi:10.1055/s-0044-101263 (2018).
6. Agrawal, M. D. et al. Improved hepatic arterial phase MRI with 3-second temporal resolution. J Magn Reson Imaging 37, 1129-1136, doi:10.1002/jmri.23920 (2013).
7. Bane, O. et al. Hemodynamic measurements with an abdominal 4D flow MRI sequence with spiral sampling and compressed sensing in patients with chronic liver disease. J Magn Reson Imaging, doi:10.1002/jmri.26305 (2018).
8. Pahwa, S. et al. Quantitative perfusion imaging of neoplastic liver lesions: A multi-institution study. Sci Rep 8, 4990, doi:10.1038/s41598-018-20726-1 (2018).
9. Gurney, P. T., Hargreaves, B. A. & Nishimura, D. G. Design and analysis of a practical 3D cones trajectory. Magn Reson Med 55, 575-582, doi:10.1002/mrm.20796 (2006).
10. Johnson, K. M., Block, W. F., Reeder, S. B. & Samsonov, A. Improved least squares MR image reconstruction using estimates of k-space data consistency. Magn Reson Med 67, 1600-1608, doi:10.1002/mrm.23144 (2012).
Figures
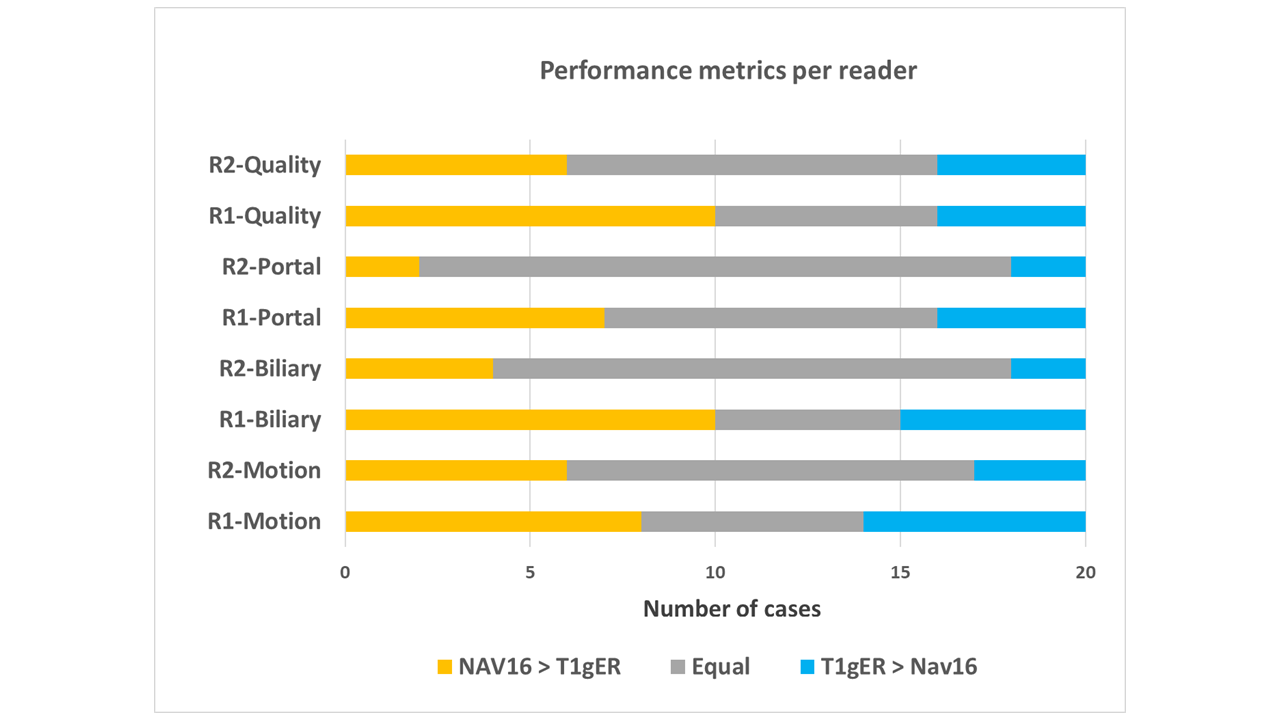
Graphical representation of reader scoring. The orange bars represent the sum of cases where Nav16 was scored higher than T1gER, blue bars represent cases where T1gER scored higher than Nav16, and the gray bar cases were they were scored equally. Datasets are organized along the y-axis, separated by both reader and scoring metric.
R1 - Reader 1; R2 - Reader 2.