1636
Motion-Corrected Proton Density-Weighted In-Phase Stack-of-Stars (PDIP SOS) FLASH MR Imaging of Kidney Stone Disease1Radiology, NorthShore University HealthSystem, Evanston, IL, United States, 2Radiology, Feinberg School of Medicine, Northwestern University, Chicago, IL, United States, 3Surgery, NorthShore University HealthSystem, Evanston, IL, United States, 4Siemens Medical Solutions USA Inc, Chicago, IL, United States, 5Radiology, University of Chicago Pritzker School of Medicine, Chicago, IL, United States
Synopsis
Kidney stones affect 1 in 11 people in the United States and renal colic resulting from obstructing stones is a frequent cause of emergency department visits. Non-contrast CT of the abdomen and pelvis is the primary imaging test but has the drawback of exposing the patient to potentially significant amounts of ionizing radiation. A motion-corrected proton density-weighted in-phase stack-of-stars (PDIP SOS) FLASH pulse sequence was developed to provide a potential imaging alternative. Using this approach, we have demonstrated for the first time the feasibility of using MRI to detect kidney stones with image quality that is competitive to CT.
INTRODUCTION
Acute renal colic is a debilitating condition caused by an obstructing kidney stone. It typically presents with severe flank pain, nausea and vomiting. Kidney stones affect 1 in 11 people in the United States1 and renal colic resulting from obstructing stones is a frequent cause of emergency department visits. While there are several different types of kidney stones, approximately 90% are composed of calcium oxalate or calcium phosphate. Non-contrast CT of the abdomen and pelvis is the primary imaging test used for initial diagnosis. It is also used to evaluate the size and location of renal and ureteral stones, which is key to patient management as this information determines the likelihood of spontaneous stone passage without surgical intervention.2 Non-contrast CT has proven highly accurate for stones >3 mm in diameter. However, the use of CT entails a substantial radiation dose, especially in patients with large BMI, and multiple CT scans are required in a subset of patients due to recurrent disease. This is particularly undesirable given the relatively young age of many of these patients, with the peak incidence for nephrolithiasis at 20–49 years.3 While MR urography can demonstrate an obstructing stone within a dilated ureter, no MR imaging technique has yet proved adequate for imaging stones within the kidneys or a non-obstructed ureter. Recently, a motion-insensitive proton density-weighted in-phase stack-of-stars (PDIP SOS) FLASH pulse sequence proved competitive to CT for the delineation of aorto-iliac and ilio-femoral vascular calcifications.4 We hypothesized that this technique, after incorporating motion correction using a diaphragm navigator or self-navigation to compensate for displacement of the kidneys during respiration, could be used to image kidney stones even in the absence of an obstructed collecting system.METHODS
This IRB-approved study was conducted in healthy volunteers and one patient with documented renal stone disease on a 3 Tesla scanner (MAGNETOM Skyrafit, Siemens Healthcare, Erlangen, Germany). Following scout imaging, a prototype PDIP SOS FLASH sequence was acquired through both kidneys with 600 to 1000 radial views, 64 to 96 slices, echo spacing = 5.0 msec, in-phase TE = 2.46 msec, flip angle = 2.5 degrees, isotropic spatial resolution ~ 1.2-mm x 1.2-mm x 1.2-mm. Motion correction was performed using a cross-pair diaphragm navigator with a 3-mm acceptance window or self-navigated retrospective respiratory gating using a 50% acceptance window. Images were viewed as 3-mm thick minimum intensity projections in multiple orientations.RESULTS
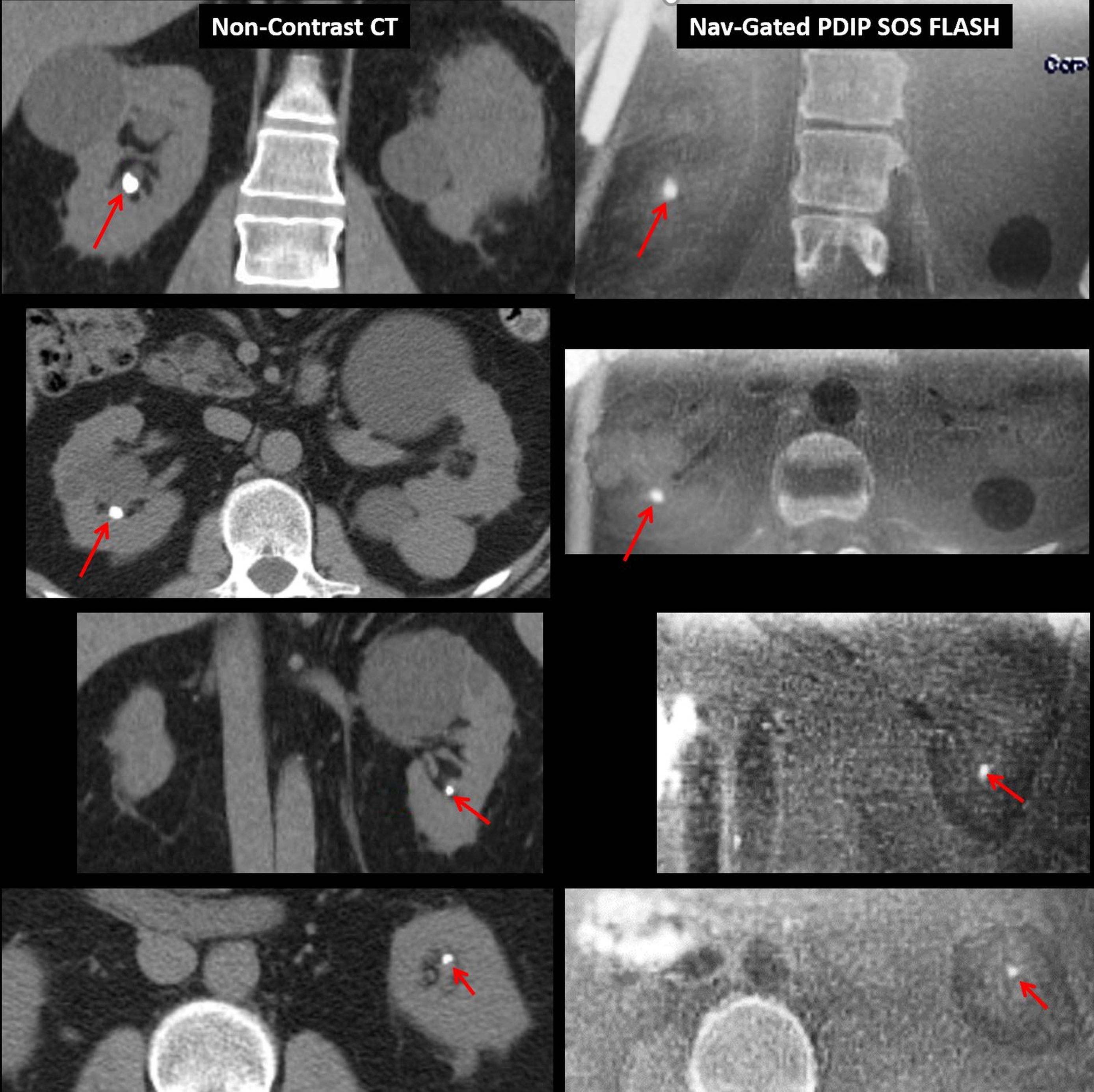
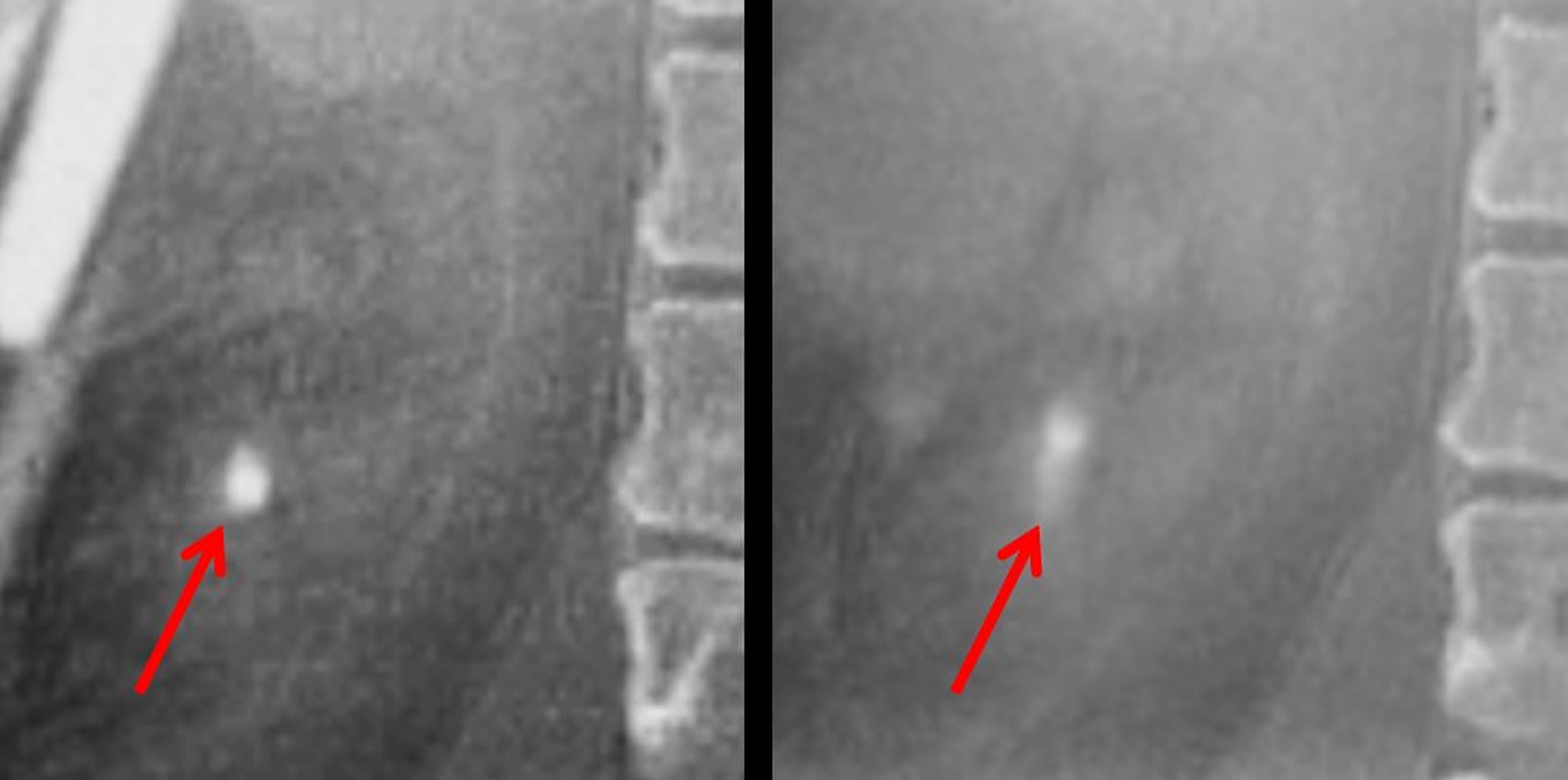
Scan time for the motion-corrected technique was approximately 10 to 12 minutes. The PDIP SOS FLASH sequence produced images in which the renal parenchymal tissues, fat, blood vessels, and ureters showed a uniform, intermediate signal intensity. In volunteers, delineation of the renal margins was substantially improved by use of motion correction. In the patient study, navigator-gated PDIP SOS FLASH demonstrated a 7-mm calculus in the right kidney and 5-mm calculus in the left kidney comparably to non-contrast CT (Figure 1). Use of motion correction substantially improved the edge definition of the calculi, particularly in the head-to-foot direction (Figure 2).DISCUSSION
Conventional MRI pulse sequences generate kidney images in which a variety of signal intensities coexist, making it problematic to confidently identify a small, low-signal kidney stone. Ultra-short TE imaging techniques have been used successfully to characterize kidney stones in vitro but not in patients. PDIP radial VIBE has several advantages for imaging of kidney stones: (1) it produces high contrast between low-signal stones and renal tissues; (2) it permits isotropic imaging with small voxels, necessary to avoid partial volume averaging between small stones and surround tissue; and (3) it suppresses artifacts from bowel motion that might otherwise obscure a small stone. Unlike the aorto-iliac vessels, which are relatively stationary, the kidneys typically move several centimeters over the course of the respiratory cycle. Consequently, it proved essential to correct for respiratory motion using either a diaphragm navigator or self-navigation, despite the intrinsic motion insensitivity of the technique.CONCLUSION
We have demonstrated for the first time the feasibility of using MRI to detect kidney stones with image quality that is competitive to CT. While further study is needed to determine the accuracy of the technique and to further improve imaging efficiency, motion-corrected PDIP SOS FLASH has the potential to eventually provide a safe, radiation-free alternative to CT in the evaluation of patients with kidney stone disease.Acknowledgements
FUNDING SOURCES: NIH grants R01 HL137920 and R01 HL130093References
1. Scales et al. Eur Urol. 2012; 62(1):160.
2. Brisbane et al. Nat Rev Urol. 2016; 13(11): 654.
3. Aggarwal et al. EMJ Urol. 2017;5(1):98.
4. Serhal et al. J Cardiovas Mag Reson. 2018; 20:15.
Figures