1631
Classification of prostate cancer by radiomics1East China normal university, Shanghai, China, 2Jiangsu Province Hospital, Jiangsu, China, 3MR Scientific Marketing, Siemens Healthcare, shanghai, China
Synopsis
Timely diagnosis and treatment could effectively reduce patient risk for clinical significant prostate cancer (PCa). In this abstract, we extracted 327 quantitative features from prostate mp-MRI images, then we used a homemade open-source tool named Feature Explorer to study combinations of radiomics algorithms and hyper-parameters in order to find the best model for classification of PCa into non-clinical–significant and clinical significant. We obtained a candidate model with AUC of 0.823, accuracy of 0.827. Four features selected for classification are easily understandable in the sense of image characteristics. Feature Explorer was demonstrated to be an efficient tool for radiomics studies.
INTRODUCTION:
Prostate cancer (PCa)
is one of the most common cancer in the world and the number of patients increased
significantly in recent years.1,2,3 Most of PCa with
Gleason score less than 7 may remain low-risk for decades, but some PCa may
deteriorate to clinical significant (CS) PCa with high fatality rate.4 Multi-parametric
magnetic resonance imaging (mp-MRI) is widely used to diagnose PCa.5 However, experienced
radiologists are often required in PCa screening with mp-MRI. In this abstract,
we extracted 327 quantitative features from the prostate mp-MRI images and
correlated them to PCa classfications.6METHODS:
Dataset: PROSTATEx (https://doi.org/10.7937/K9TCIA.2017.MURS5CL) dataset was used in this study. It included 185 cases with T2W(TSE,0.5×0.5×3.6mm3), DWI(SSEP,2×2×3.6mm3,b is 800s/mm2), and ADC map sequences from Siemens 3T MR scanners. Total 251 lesions (CS/NCS=68/183) were used in this study. DWI and ADC map were aligned to T2W images. A radiologist drew the region of interest (ROI) manually. We split the dataset into independent training (CS/NCS = 48/128) and testing dataset (CS/NCS = 20/55).
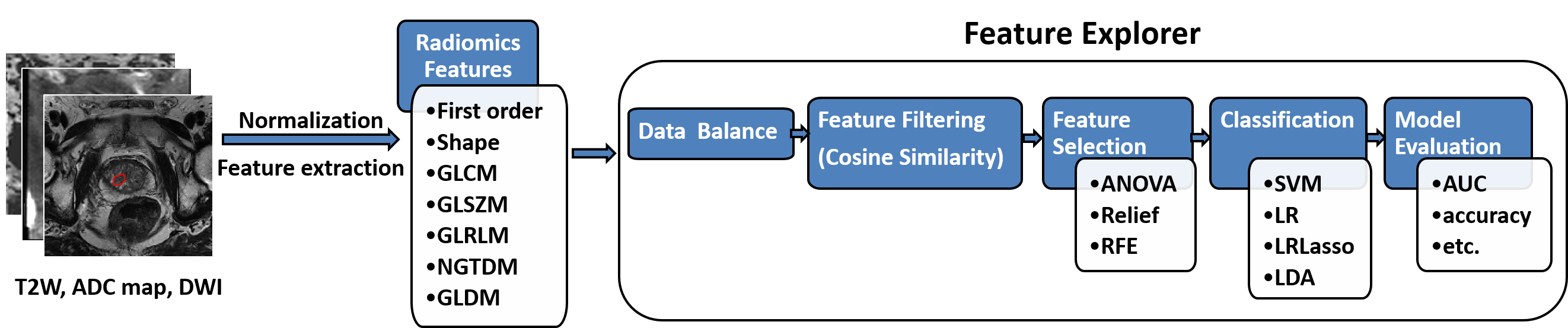
Radiomics Feature Extraction: We extracted 109 features from each ROI in each sequence with pyradiomics (http://pyradiomics.readthedocs.io/en/latest/index.html). Classes of the features used included Shape (19), First Order (16), Gray Level Co-occurrence Matrix (GLCM, 23), Gray Level Size Zone Matrix (GLSZM, 16), Gray Level Run Length Matrix (GLRLM, 16), Neighboring Gray Tone Difference Matrix (NGTDM, 5), Gray Level Dependence Matrix (GLDM, 14).
Feature Explore Pipeline: Since there are numerous number of combinations of algorithms and hyper-parameters to try out to find the best model for classification, we used a homemade open-source tool named Feature Explorer (FAE, https://github.com/salan668/FAE) to automate the process. We normalized each features, and used upsampling for data balance. Then we tried out all the combinations of three feature selection methods (ANOVA, Relief, and Recursive feature elimination) and four classifiers (SVM, LDA, Logistic Regression, and Logistic Regression with Lasso). Number of selected features was also iterated from 1 to 20. The best model was found by comparing the results of leave-one-out cross validation on the training dataset. Finally, we used receiver operating characteristic curve (ROC), area under ROC (AUC), paired t-test on the testing dataset to quantitatively evaluate the performance of the best model.
RESULTS:
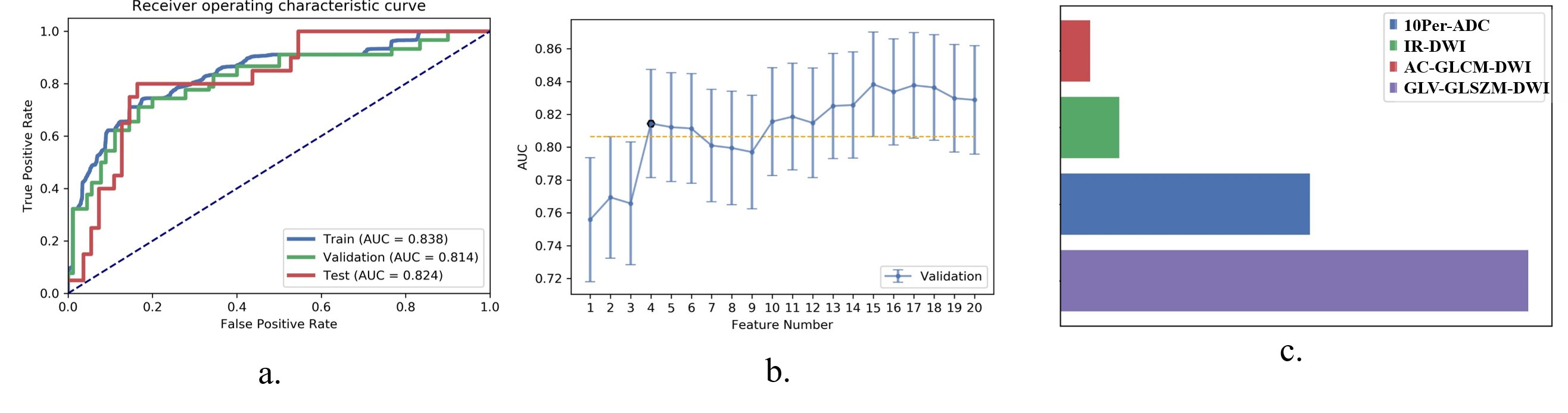
We found
that the combination of ANOVA and LDA with 4 features selected yielded the best
results, with AUC of 0.823, accuracy of 0.827, sensitivity of 0.800, specificity
of 0.836, positive predictive value of 0.640, negative predictive value of 0.920.
We showed the ROC curve of the model on training/validation/testing dataset in
Figure 2 (a). The plot of the AUC on validation dataset against the number of
features was shown in Figure 2 (b). The candidate number of features was determined
with one-standard-error rule. The selected features were: (1) 10th percentile of ADC map (10Per-ADC),
(2) the interquartile range of intensity analysis of DWI (IR-DWI), (3) auto-correlation
of GLCM of DWI (AC-GLCM-DWI), and (4) the gray level variance of GLSZM of DWI
(GLV-GLSZM-DWI). The contributions of these four features in the final model
were shown in
Figure
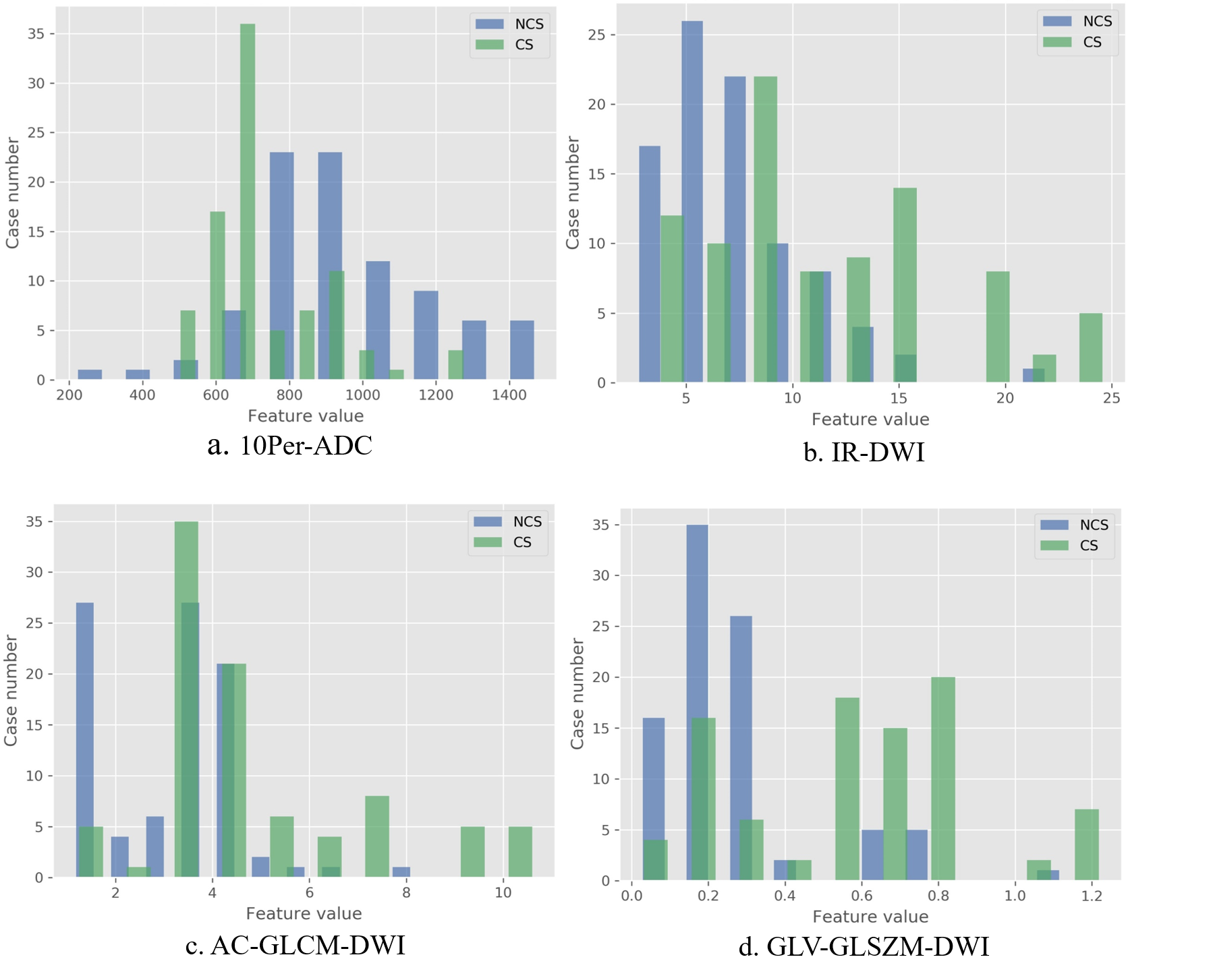
2. We also showed
the distribution of these features of both CS and NCS PCa in Figure 3. The
p-value of these features was smaller than 0.001 to distinguish the CS and NCS
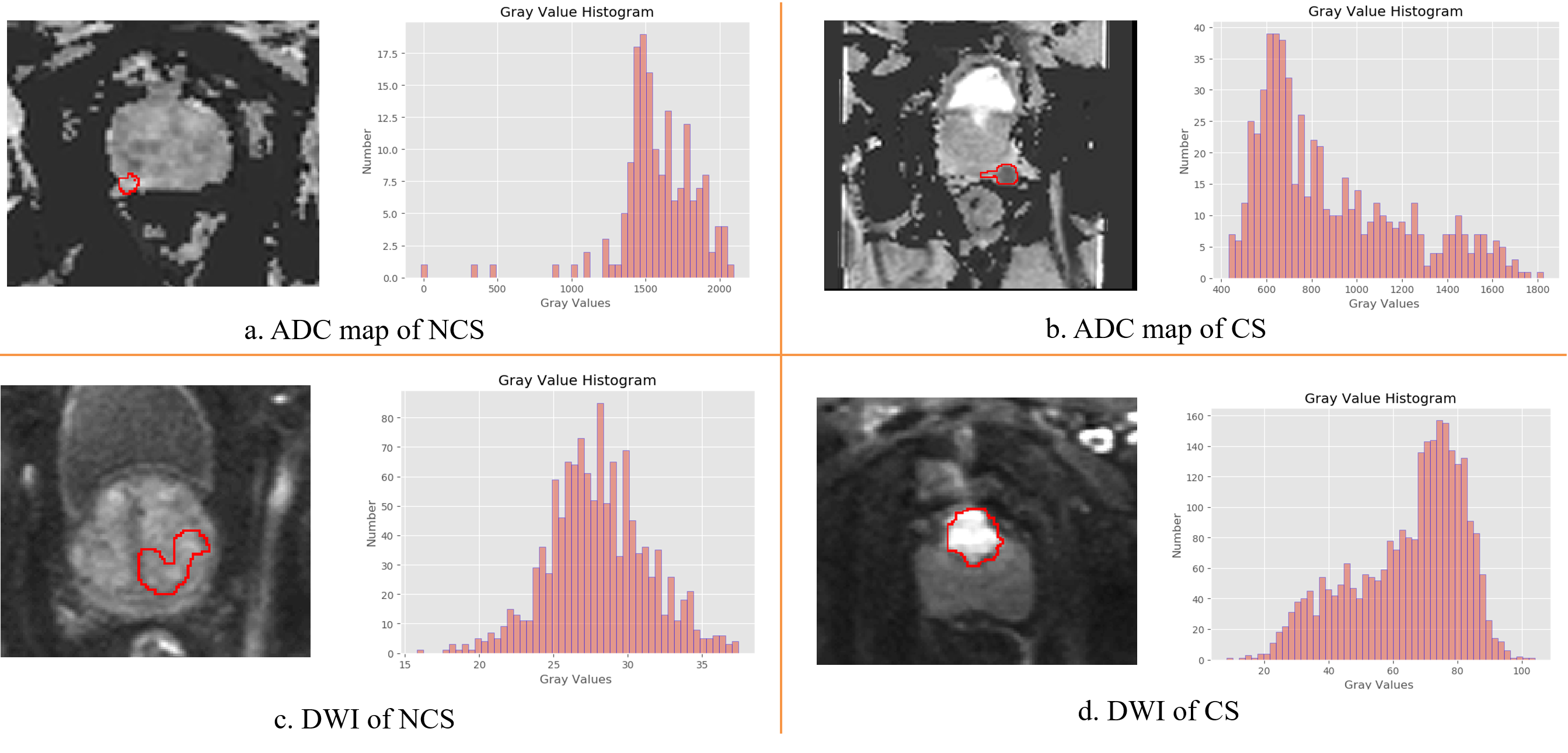
PCa. The histogram within ROI of CS and NCS PCa cases were shown in Figure 4.
The features related to the histogram could be used to separate the CS and NCS
PCa.
DISCUSSION:
The intensity of PCa
is higher in DWI image and lower in ADC. However, to separate CS from NCS, more
complex features need to be used. From the radiomics analysis, we found 10Per-ADC and IR-DWI could be used to
separate CS and NCS PCa. From Figure 4 (a) and (b), we can see that the
skewness of NCS and CS are negative and positive respectively. AC-GLCM-DWI, which reflected
fineness and coarseness of texture, had
higher values in DWI of CS PCa, indicating CS PCa tends to have coarser
texture.
GLV-GLSZM-DWI is also higher in CS,
which means CS
PCa is more inhomogeneous in gray
level intensities. Though none of the above features can separate CS
from NCS, the model combining all these 4 features could help to diagnose the
CS PCa. CONCLUSION:
With the help of a
homemade radiomics software, Feature Explorer, we found the best model for PCa classification.
Four features, each associated with certain image characteristics and easily
understandable, were found to be most relevant to CS/NCS classification. Acknowledgements
This project is supported by National Natural Science Foundation of China (81771816,61731009).References
1.Canadian Cancer Society, Prostate Cancer Statistics, 2015.
2.American Cancer Society, Cancer Facts & Figures 2015.
3.A. Jemal, F. Bray, M. M. Center, J. Ferlay, E. Ward, and D. Forman, CA: a cancer journal for clinicians: Global cancer statistics, 2011; vol. 61, no. 2, pp. 69–90.
4.A. Stangelberger, M. Waldert, and B. Djavan, Prostate cancer in elderly men, Rev. Urol, 2008; vol. 10, no. 2, pp. 111–119.
5.Y. Peng et al. Quantitative analysis of multiparametric prostate MR images: Differentiation between prostate cancer and normal tissue and correlation with Gleason score—A computer-aided diagnosis development study, Radiology, 2013; vol. 267, no. 3, pp. 787–796.
6.P. Lambin, E. Rios-Velazquez, R. Leijenaar, S. Carvalho, et al. Radiomics: extracting more information from medical images using advanced feature analysis, European Journal of Cancer, 2012; vol. 48, no. 4, pp. 441–446.
Figures