1624
Automatic detection of prostate cancer lesion using various deep neural network in multi-parametric MRI combined including quantified parameters.1AI R&D Center, JLK Inspection, Seoul, Korea, Republic of, 2Department of Radiology, Asan Medical Center, Seoul, Korea, Republic of
Synopsis
we used qualitative and quantitative parametric MRI in various deep convolutional neural networks for fully-automatic detection of prostate cancer. region. various deep neural networks were compared with pathology map-based ground truth. The 3D convolutional neural networks achieved the highest performance in our experiments.
Introduction
Multi-parametric magnetic resonance image (mp-MRI) is widely used for detection and staging of prostate cancer [1-3]. Currently, comprehensive interpretation of T2-weighted(T2w) images, diffusion-weighted images (DWI), dynamic contrast-enhanced MRI (DCE-MRI) image can provide a greater diagnostic accuracy than single-modal MRI [1-3]. However, visual inspection of mp-MRI requires a significant training period, and moreover may be inconsistent between or within observers. This potential limitation can be overcome by using computer-aided diagnosis tool such as support vector machine and multi-layer perceptron [4-5]. In this paper, we propose convolutional neural network (CNN)-based automatic segmentation methods to detect prostate cancer in qualitative and quantitative mp-MRI. We compared the diagnostic performance among various 2D CNN and 3D CNN methods using receiver operating characteristic (ROC) curve. AUC value obtained with 3D CNN method were higher than those with the other 2D CNN methods.Method
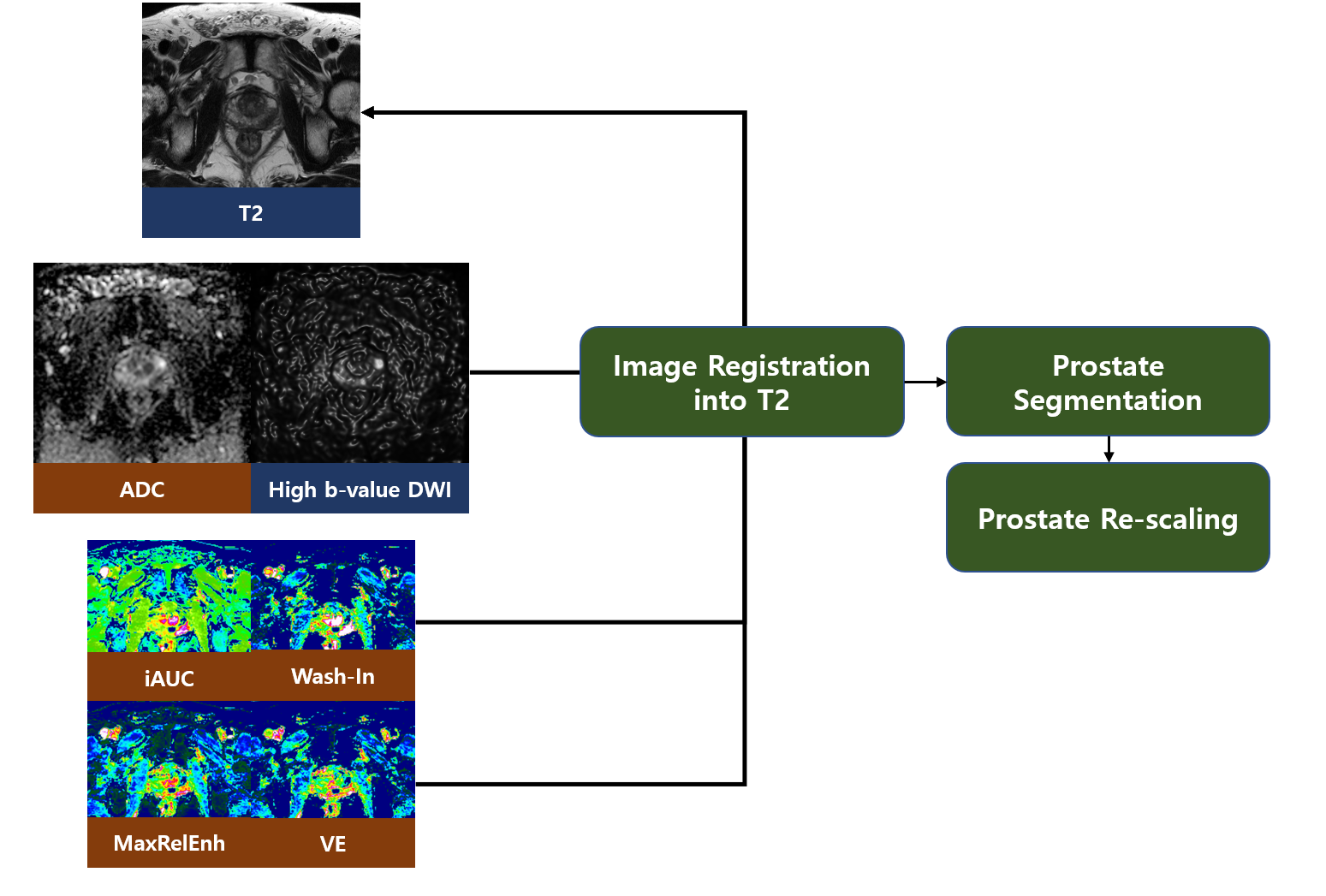
mp-MRIs and pathology maps obtained from 350 patients who underwent radical prostatectomy. The mp-MRI included multi-slice T2w images, DWI images, and DCE-MRI. Apparent diffusion coefficient (ADC) map and high b-value DWI images at b value of s/mm2 were calculated from DWI images. Also, four parametric maps were generated form DCE MRI, including arear under time-intensity curve(iAUC), Extracellular volume ratio reflecting vascular permeability (VE), Wash-in rate (Wash-in), and peak enhancement ratio (MaxRelEnh). For setting ground truth for training and validation process, an experienced radiologist labelled cancer lesion greater than 5 mm in diameter by referring to histological map. The qualitative and quantitative images were used as input data to generate voxel-based probability map for prostate. T2w, ADC, b1500, iAUC, VE, Wash-in and MaxRelEnh were used for input images of our deep neural network because they have been used to diagnose prostate cancer in clinical site [6-7]. Figure 1 shows the acquisition process of mp-MRI images. In training process, the annotated ground truth images were used for the output of our deep neural networks. In validation process, the images were used to evaluate performances of our proposed neural networks. Some pre-processing algorithms were used into the mp-MRI images. First, the other mp-MRI images were registered into high quality and resolution T2w. Next, prostate regions were segmented by our CNN based deep neural network. Finally, the re-scale algorithm was used into the prostate region of mp-MRIs. The enlarged prostate images were used in our proposed deep neural network for cancer segmentation. Figure 2 shows our pre-processing flow-work The number of our convolutional neural networks [11-15] for prostate cancer segmentation was eleven, as it can be shown in figure 3. We included multi parametric input image processing layer in each network. The mp-MRI and ground truth images of 300 patients were used in training process, and those of 50 patients used in validation process.Results
For the quantitative validation of our networks, the mp-MRI images and ground truth of mid-gland prostate were divided into four regions [8-10]. The segmentation results of our deep neural networks were compared with the divided ground truth images. Sensitivity (true positive) and specificity (false negative) values were calculated from the comparison. Also, the ROC curves and AUC values were obtained from various cutoff values of segmentation probability. Figure 4 shows the ROC curves of our proposed networks. In the case of 2D networks, The AUC value of PCD was higher than that of the other networks. PCD networks used DCE parameters processing layer. Because the information of DCE-MRI was different with the that of the other parametric images, DCE parameter process layer separated with the other parametric MRI in PCD network leads to good performance for prostate cancer detection The 3D networks, which AUC value was 0.93, outperformed other 2D networks. Cancer tends to develop 3D shape in the prostate region. While 2D networks cannot consider the correlation between adjacent slices and 3D cancer shape, 3D networks can consider the correlation and the cancer shape.Conclusion
In this paper, we used qualitative and quantitative parametric MRI in various deep neural networks for automatic detection of prostate cancer. eleven convolutional neural networks were compared with pathology map-based ground truth. The 3D networks achieved the highest performance in our experiments.Acknowledgements
No acknowledgement found.References
[1] Weinreb, Jeffrey C., et al. "PI-RADS prostate imaging–reporting and data system: 2015, version 2." European urology 69.1 (2016): 16-40.
[2] Ahmed, Hashim U., et al. "Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study." The Lancet 389.10071 (2017): 815-822.
[3] Hamoen, Esther HJ, et al. "Use of the Prostate Imaging Reporting and Data System (PI-RADS) for prostate cancer detection with multiparametric magnetic resonance imaging: a diagnostic meta-analysis." European urology 67.6 (2015): 1112-1121.
[4] Guo, Yanrong, Yaozong Gao, and Dinggang Shen. "Deformable MR prostate segmentation via deep feature learning and sparse patch matching." IEEE transactions on medical imaging 35.4 (2016): 1077-1089.
[5] Yang, Xin, et al. "Co-trained convolutional neural networks for automated detection of prostate cancer in multi-parametric MRI." Medical image analysis 42 (2017): 212-227.
[6] Kim, Jeong Kon, et al. "Wash‐in rate on the basis of dynamic contrast‐enhanced MRI: usefulness for prostate cancer detection and localization." Journal of Magnetic Resonance Imaging: An Official Journal of the International Society for Magnetic Resonance in Medicine 22.5 (2005): 639-646.
[7] Sung, Yu Sub, et al. "Dynamic contrast‐enhanced MRI for oncology drug development." Journal of Magnetic Resonance Imaging 44.2 (2016): 251-264.
[8] Vargas, Hebert Alberto, et al. "Diffusion-weighted endorectal MR imaging at 3 T for prostate cancer: tumor detection and assessment of aggressiveness." Radiology 259.3 (2011): 775-784.
[9] Brock, M., et al. "Fusion of magnetic resonance imaging and real-time elastography to visualize prostate cancer: a prospective analysis using whole mount sections after radical prostatectomy." Ultraschall Med 36 (2015): 355-361.
[10] Lim, Hyun Kyung, et al. "Prostate cancer: apparent diffusion coefficient map with T2-weighted images for detection—a multireader study." Radiology 250.1 (2009): 145-151.
[11] Long, Jonathan, Evan Shelhamer, and Trevor Darrell. "Fully convolutional networks for semantic segmentation." Proceedings of the IEEE conference on computer vision and pattern recognition. 2015.
[12] Wolterink, Jelmer M., et al. "Dilated convolutional neural networks for cardiovascular MR segmentation in congenital heart disease." Reconstruction, Segmentation, and Analysis of Medical Images. Springer, Cham, 2016. 95-102.
[13] Chen, Hao, et al. "VoxResNet: Deep voxelwise residual networks for brain segmentation from 3D MR images." NeuroImage (2017).
[14] Ronneberger, Olaf, Philipp Fischer, and Thomas Brox. "U-net: Convolutional networks for biomedical image segmentation." International Conference on Medical image computing and computer-assisted intervention. Springer, Cham, 2015.
[15] Li, Xiaomeng, et al. "H-DenseUNet: Hybrid Densely Connected UNet for Liver and Tumor Segmentation from CT Volumes." IEEE Transactions on Medical Imaging (2018).
Figures