1623
Prostate cancer detection using an integrated slice-by-slice shimming acquisition scheme and three MR diffusion models: correlation with in-bore transperineal MR-guided biopsy1The First Affiliated Hospital of Soochow University, suzhou, China, 2MR Application Development, Siemens Healthcare, Erlangen, Germany, Erlangen, Germany, 3MR Scientific Marketing, Siemens Healthcare, Shanghai, SHANG HAI, China
Synopsis
Multiparametric magnetic resonance imaging (mpMRI) of the prostate gland is increasingly being used in the setting of newly diagnosed disease to identify occult, higher-grade, or stage elements missed by conventional biopsy. In this study, a prototype diffusion weighted single shot EPI sequence with integrated slice-by-slice shimming (iShim) technique was applied to reduce the susceptibility artifacts of DW images[1]. Conventional mono-exponential DWI, intravoxel incoherent motion (IVIM), and diffusional kurtosis imaging (DKI) models were applied to preoperatively predict prostate cancer (PCa)[2, 3]. Our research showed that the diffusion coefficient in the peripheral zone, mean kurtosis, and the PSA level in the transition zone are potential predictive biomarkers for PCa.
Purpose
To evaluate the potential role of standard diffusion-weighted imaging (DWI), intravoxel incoherent motion (IVIM), and diffusional kurtosis imaging (DKI) findings for the preoperative prediction of prostate cancer (PCa) by using a prototype diffusion weighted single shot EPI sequence with integrated slice-by-slice shimming technique (iShim).
Methods
The study was approved by the institutional review board. A total of 81 consecutive patients were enrolled from May 2017 to February 2018 (27 cases of PCa and 54 cases of non-PCa). All the exams were performed on a 3T scanner (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). The b-value DWI data were acquired using the iShim technique with b-values ranging from 0 to 2100 s/mm2. Different b-value combinations were selected to fit the conventional mono-exponential diffusion model, IVIM (50, 100, 200, 700, 1400 and 2100 sec/mm2) and DKI (0, 700, 1400, and 2100 s/mm2), and the corresponding diffusion parameter maps were generated using a prototype software (Body Diffusion Toolbox, Siemens Healthcare, Erlangen, Germany). Univariate and multivariate logistic regression analyses were used to evaluate the relative value of these diffusion parameters as potential predictors of PCa. The results were compared with the findings of in-bore transperineal MR-guided biopsy.Results
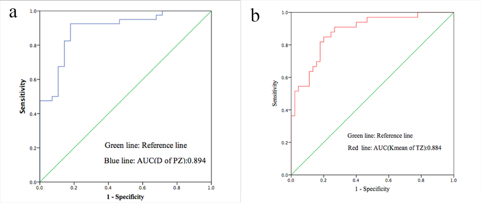
The features significantly related to PCa included decreased ADC (P < 0.05), Dmean (P < 0.05), D (P < 0.05), and increased Kmean (P < 0.05) in the peripheral zone (PZ), and increased Kmean (P < 0.05), decreased ADC (P < 0.05), Kmean (P < 0.05), Dmean (P < 0.05), and prostate-specific antigen (PSA) level (P = 0.011) in the transitional zone (TZ). In the multivariate analysis, decreased D (P = 0.015; odds ratio, 0.99; 95% CI: 0.99, 1.00) was an independent risk factor for PCa in the PZ, and the PSA level (P = 0.014; odds ratio, 1.08; 95% CI: 1.02, 1.15) and Kmean (P = 0.018; odds ratio, 1.01; 95% CI:1.00, 1.02) were independent risk factors for PCa in the TZ. The decreased D showed an area under the receiver operating characteristic curve of 0.894 (optimal cutoff value was 1.33 × 10-3 mm2/sec) in the PZ, and the increased Kmean of 0.884 (optimal cutoff value was 0.87 × 10-3 mm2/sec) in the TZ.Conclusions
By using the iShim DWI sequence and three diffusion models(ADC, IVIM, and DKI), the results of this study showed that the calculated D value from the IVIM model for the PZ, Kmean map, and PSA level for the TZ are potential predictive biomarkers for PCa.Acknowledgements
No acknowledgement found.References
1. Zhang, H, H Xue, S Alto, et al, Integrated Shimming Improves Lesion Detection in Whole-Body Diffusion-Weighted Examinations of Patients With Plasma Disorder at 3 T. Investigative Radiology, 2015: p. 1.
2. Roethke, M C, T A Kuder, T H Kuru, et al, Evaluation of Diffusion Kurtosis Imaging Versus Standard Diffusion Imaging for Detection and Grading of Peripheral Zone Prostate Cancer. Invest Radiol, 2015. 50(8): p. 483-9.
3. Wang, W T, L Yang, Z X Yang, et al, Assessment of Microvascular Invasion of Hepatocellular Carcinoma with Diffusion Kurtosis Imaging. Radiology, 2018. 286(2): p. 571-580.
Figures