1620
Joint estimation of the field inhomogeneity and geometrical distortion for quantitative susceptibility mapping of the prostate1Ryerson University, Toronto, ON, Canada, 2Sunnybrook Research Institute, Toronto, ON, Canada, 3University of Toronto, Toronto, ON, Canada
Synopsis
The geometrical distortions of MR images are potential source of error in MR-based radiation therapy planning (RTP) which requires accurate anatomical delineation. Beside the system-specific residual distortions, presence of any susceptibility-mismatch within the region of interest may lead to image distortion. We have recently proposed an algorithm based on quantitative susceptibility mapping (QSM) for post-implant dosimetry of prostate brachytherapy seeds. In this study, the undistorted field map in patients with and without implanted seeds was estimated and images were corrected accordingly, then QSM was performed. In patients with implanted seeds, distortion correction improved the accuracy of the QSM reconstruction.
Introduction
The geometrical distortion on MR images arise from either residual system-specific distortion in field inhomogeneity (B0) and transmit field (B1) non-linearity or patient-induced distortions. Field inhomogeneities typically result in both, geometric distortions and intensity corruption of the MR images. The patient susceptibility-induced distortions are of major concern where any susceptibility mismatch such as air cavities are presents within the region of interest. In prostate MRI, presence of air in the rectum or bowels may result in field-induced image distortion and artefacts1. In MRI-based radiation therapy treatment planning, a few millimeters of distortion may result in significant error in target delineation and dose calculation hence field inhomogeneity-induced geometrical distortions and intensity artifacts needs to be accounted for in MR-based radiation treatment planning. Recently, it has been shown that patient induced distortions are significantly larger than those from the system residuals in prostate cancer patients2. Low-dose-rate (LDR) brachytherapy for prostate cancer involves permanent implantation of several radioactive seeds within prostate, each encapsulated in a cylindrical titanium shell (4.5mmx0.8mm). The quality of an implantation is evaluated through post-implant dosimetry which is commonly done using CT imaging. We have recently proposed an MRI-based workflow based on QSM3 . However, the proposed method in patients resulted in maximum offset of 3.5mm between CT and MR-derived seed positions. In this study, we calculated the undistorted field map and corrected the gradient recalled echo (GRE) images for distortions and intensity corruptions prior to susceptibility mapping for seed visualization and detection.
Methods
One prostate patient with 78 implanted brachytherapy seeds and two healthy volunteers were scanned with a 3D multi echo GRE pulse sequence on 1.5T (Philips Ingenia) and 3T (Philips Achieva) scanners using a torso coil. The water-fat in-phase TEs at each field strength was used. To achieve the desired spatial resolution for seed depiction and to minimize the effect of distortion a high readout bandwidth was used (976Hz/px on 1.5T and 1240Hz/px on 3T).
The undistorted field map estimation and image correction were performed in k-space domain. The k-space data, $$$y(t)$$$ and the system matrix, $$$A(\omega,t)$$$ were calculated from complex input images using the MIRT toolbox4. The method of Matakos et. al. for joint estimation of undistorted field map, $$$\omega$$$ and corrected images, $$$\delta$$$ was used to estimate the undistorted field map by iteratively solving the following optimization problem5:
$$\omega^{k+1}=argmin_{\delta,\omega}\parallel y(t)-A(\omega^{k},t)\delta^{k}\parallel_2^2 +\lambda_{i}\parallel c_{i}\delta^{k}\parallel_2^2 +\lambda_{f}\parallel c_{f}\omega^{k}\parallel_2^2$$
An initialization for the field map was introduced as the normalized difference between two consecutive distorted phase images to the ∆TE. The complex images were corrected according to the estimated undistorted field map () by solving the following non-linear optimization problem via the preconditioned conjugate gradients (PCG) algorithm6–8:
$$\delta^{k+1}=argmin_{\delta}\parallel e^{y(t)}-e^{A(\omega,t)\delta^{k}} \parallel_2^2 +\lambda_{i}\parallel c_{i}\delta^{k}\parallel_2^2 $$
The corrected complex images were used to perform QSM with morphology enabled dipole inversion (MEDI) using the method explained in Refs. 3,9–11 by solving the following optimization problems:
$$\chi_{r}=argmin_{\chi_{r}}\lambda\parallel W[e^{iD_{r}\chi_{r}} - e^{if_{r}}]\parallel_2^2 +\parallel G_{M}G_{\chi}\parallel_{1}$$
Patient and volunteers were also CT scanned and the seed positions on CT images were used as reference points to compare the QSM results with and without distortion correction.
Results and Discussion
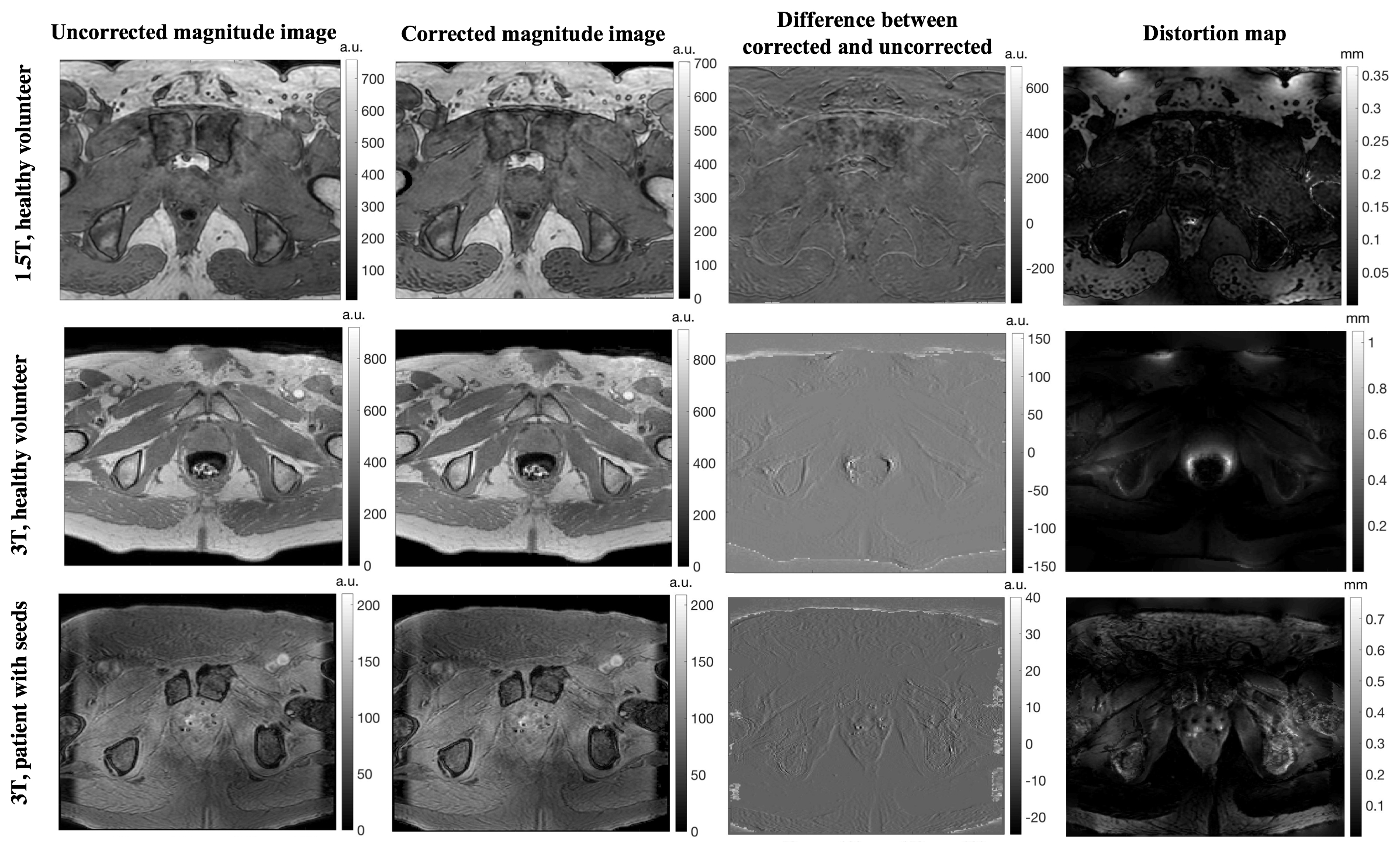
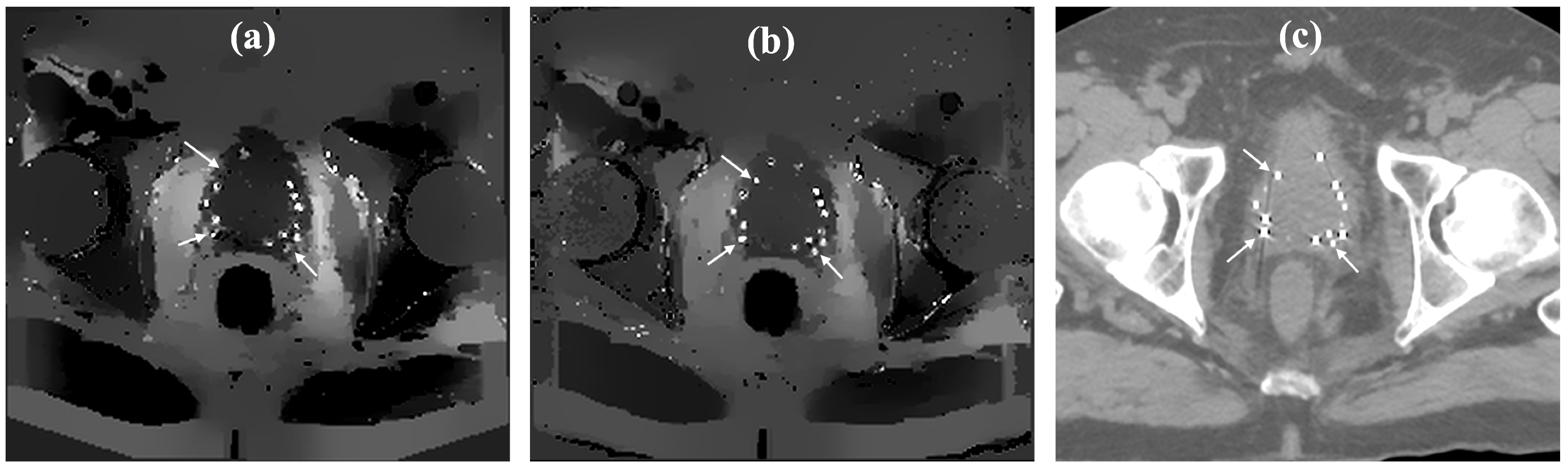
The effect of geometrical distortion correction algorithm on healthy volunteers at 1.5T and 3T as well as in the patient with implanted seeds on 3T are shown in Fig.1. The distortion maps (calculated as the undistorted field map normalized to the readout bandwidth) demonstrated in Fig.1 shows that for non-seeded prostates, the maximum distortions were 0.4mm and 1.2mm at 1.5T and 3T respectively which were observed mainly at the interface between rectum and prostate; However, in the patient with implanted seeds the maximum distortion of 1.1mm was observed around the seeds. The observed distortions for non-implanted prostates will not result in significant difference in dosimetric analysis1. However, the distortion around the seeds were within the seeds dimensions and resulted in significant error in spatial accuracy of the seed reconstruction through MEDI-QSM. Fig.2 shows the estimated QSM using the original distorted and distortion-corrected complex GRE images. Although all the seeds were reconstructed through QSM using distorted images, the distortion correction significantly improved the spatial accuracy of the reconstructed seeds positions which is critical for seed localization and dose calculations. With no correction applied the maximum and mean Euclidian distance between CT and MR-derived seed centroids were 3.5mm and 1.2mm; distortion correction reduced the differences to 1.8mm and 0.8mm respectively. In addition, correction of the intensity corruption resulted in artifacts reduction and more uniform prostate QSM reconstruction.Conclusion
The correction of the field induced distortions and intensity corruptions is critical for MRI-based post-implant dosimetry of prostate brachytherapy.Acknowledgements
No acknowledgement found.References
1. Gustafsson, C., Nordström, F., Persson, E., Brynolfsson, J. & Olsson, L. E. Assessment of dosimetric impact of system specific geometric distortion in an MRI only based radiotherapy workflow for prostate. Phys Med Biol 62, 2976–2989 (2017).
2. Adjeiwaah, M. et al. Quantifying the Effect of 3T Magnetic Resonance Imaging Residual System Distortions and Patient-Induced Susceptibility Distortions on Radiation Therapy Treatment Planning for Prostate Cancer. Int J Radiat Oncol 100, 317–324 (2018).
3. Nosrati, R. et al. MRI-based automated detection of implanted low dose rate (LDR) brachytherapy seeds using quantitative susceptibility mapping (QSM) and unsupervised machine learning (ML). Radiother Oncol (2018). doi:10.1016/j.radonc.2018.09.003
4. Fessler, J. A. Michigan Image Reconstruction Toolbox. Available at: https://web.eecs.umich.edu/~fessler/code/. (Accessed: 10th August 2018)
5. Matakos, A. & Fessler, J. A. Joint estimation of image and fieldmap in parallel MRI using single-shot acquisitions. in 2010 IEEE International Symposium on Biomedical Imaging: From Nano to Macro 984–987 (IEEE, 2010). doi:10.1109/ISBI.2010.5490153
6. Matakos, A., Balter, J. & Cao, Y. Estimation of geometrically undistorted B0 inhomogeneity maps. Phys Med Biol 59, 4945–4959 (2014).
7. Fessler, J. A. & Xed, T. E. Conjugate-Gradient Preconditioning Methods: Numerical Results. (1997). 8. Fessler, J. A. & Rogers, W. L. Spatial resolution properties of penalized-likelihood image reconstruction: space-invariant tomographs. IEEE Trans Image Process 5, 1346–1358 (1996).
9. Liu, T. et al. Morphology enabled dipole inversion (MEDI) from a single-angle acquisition: comparison with COSMOS in human brain imaging. Magn Reson Med 66, 777–83 (2011).
10. Liu, T. et al. Nonlinear formulation of the magnetic field to source relationship for robust quantitative susceptibility mapping. Magn Reson Med 69, 467–476 (2013).
11. Liu, T. et al. A novel background field removal method for MRI using projection onto dipole fields (PDF). NMR Biomed 24, 1129–1136 (2011).
Figures