1434
Safety of Intrathecal Administration of Gadolinium-based Contrast Agents – A Systematic Review and Meta-analysisMihilkumar Patel1,2 and Santanu Chakraborty1,3
1University of Ottawa, Ottawa, ON, Canada, 2The Ottawa Hospital, Ottawa, ON, Canada, 3Neuroradiology, The Ottawa Hospital, Ottawa, ON, Canada
Synopsis
Visualizing CSF related disease processes using MRI requires the use of intrathecally administered Gadolinium-based Contrast Agents (GBCAs). MR cisternogram with GBCAs has shown to provide superior image quality compared to CT cisternogram. However, the lack of sufficient safety evidence limits its use to an off-label use. To address this, we performed a systematic review and meta-analysis to explore adverse events after intrathecal GBCA exposure. Based on our analysis, the overall incidence of serious adverse events was 2.24% with lower incidence at lower doses. We conclude that intrathecal use of GBCAs for MR imaging is safe at low doses.
Introduction
Intravenously administered Gadolinium-based Contrast Agents (GBCAs) are widely used in Magnetic Resonance imaging (MRI) procedures in order to improve lesion detection. Although conventional MRI with contrast is useful in detecting central nervous system lesions, complex CSF related disease processes are often poorly visualized without intrathecal administration of GBCAs[1]. While the adverse effects and overall safety of intravenous GBCA administration in humans has been well explored[2-3], very few studies have explored the safety profile of intrathecal administration of GBCA. There is evidence that intrathecal GBCA use in MR cisternogram studies provides greater contrast resolution than CT cisternograms[4]. However, the lack of sufficient safety evidence means intrathecal GBCA use is not approved worldwide and is currently used as an off-level use in selected patients with their consent. This study aims to fills this gap through a systematic literature review and meta-analysis to determine the rates and type of adverse events in patients after intrathecal GBCA use.Methods
A systematic literature search was conducted in MEDLINE, EMBASE, CINAHL, and the Cochrane Central Register of Controlled Trials (CENTRAL) using MeSH and keyword variations on GBCAs and intrathecal injections. Data extraction from included studies focused on rates and types of adverse events after intrathecal GBCA use. Additional data on the patient population, dose, and type of GBCA administered for each patient were also collected. The incidence of adverse events was calculated by dividing the number of patients with reported side effects by the total number of patients receiving intrathecal gadolinium. Two-tailed Chi-Square and Fisher’s exact tests were used to compare rates of adverse events across different GBCAs and doses.Results
Out of the 427 identified studies in the initial search, 52 studies with a combined total of 1028 patients were included for analysis. We identified six types of GBCA used and divided the patients accordingly: Gadopentate dimeglumine (Magnevist, n = 899), Gadobutrol (Gadovist/Gadavist, n = 95), Gadodiamide (Omniscan, n = 31), Gadobenate dimeglumine (MultiHance, n = 2), and Gadoterate meglumine (Dotarem, n = 1). The most common side effect after intrathecal administration of gadolinium was a transient, postural headache lasting 24 hours. The overall incidence of adverse events including headaches was 12.74%. When postural headaches were excluded, the incidence of adverse events was 2.24%. Meta-analysis revealed no significant difference in incidence across the different types of GBCAs when transient, postural headaches were excluded. A significant association between GBCA dose and adverse events was noted with a significant increase in adverse events with any dose greater than 1 mmol when compared with a dose less than 1 mmol (100% vs. 2.05%, p < 0.001).Discussion and Conclusion
Overall, intrathecally administered GBCAs have a low incidence of serious adverse events (2.24%), a rate that is further reduced at lower doses. Based on our analysis of the currently available literature, a safe dose range for intrathecal GBCA administration is any dose less than or equal to 1 mmol. Any dose greater than 1 mmol significantly increases the risk of serious adverse events. Among the various GBCAs studied, Gadobutrol seems to have the lowest overall side effects rate at 1.1%. However, when postural headaches are excluded, there is no significant difference among the various GBCAs, suggesting that linear agents such as Gadopentate (Magnevist) and Gadodiamide (Omniscan) may cause higher rates of postural headaches than macrocyclic agents such as Gadobutrol (Gadovist). It is important to note that while Gadopentate has been studied extensively, other GBCAs are currently limited in patient data.Acknowledgements
No acknowledgement found.References
-
Munoz
A, Hinojosa J, Esparza J. Cisternography and Ventriculography Gadopentate
Dimeglumine – Enhanced MR Imaging in Pediatric Patients : Preliminary
Report. Ajnr Am J Neuroradiol. 2007;(May):889-894.
- Zeng Q, Xiong L, Jinkins JR, Fan Z, Liu Z. Intrathecal gadolinium-enhanced MR myelography and cisternography: A pilot study in human patients. Am J Roentgenol. 1999;173(4):1109-1115. doi:10.2214/ajr.173.4.10511188
- Siebner HR, Gräfin von Einsiedel H, Conrad B. Magnetic resonance ventriculography with gadolinium DTPA: Report of two cases. Neuroradiology. 1997;39(6):418-422. doi:10.1007/s002340050436
- Delgaudio JM, Baugnon KL, Wise SK, Patel ZM, Aiken AH, Hudgins PA. Magnetic resonance cisternogram with intrathecal gadolinium with delayed imaging for difficult to diagnose cerebrospinal fluid leaks of anterior skull base. Int Forum Allergy Rhinol. 2015;5(4):333-338. doi:10.1002/alr.21475
Figures
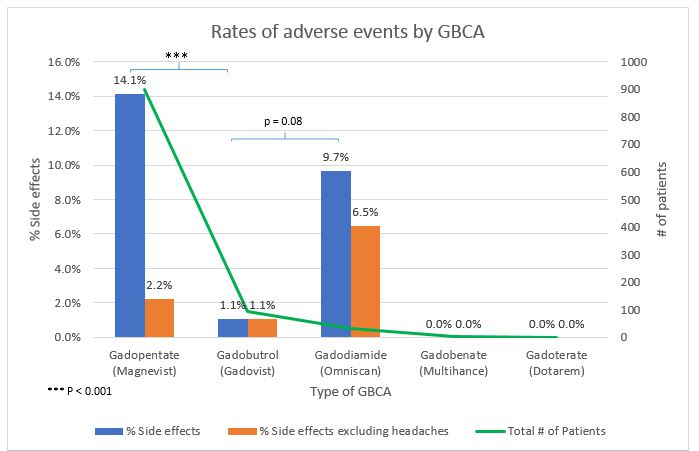
Figure 1. Comparing the overall rates of adverse events
(blue) among the
different GBCAs reveals a significant difference (p < 0.001) in side effect
rates between Gadopentate and Gadobutrol agents, with Gadobutrol yielding lower
rates of adverse events. A similar difference is found between Gadodiamide and
Gadobutrol, although the difference does not reach significance. When
transient, postural headaches are removed from the side effects (orange), there is no significant
variation among GBCAs. Gadobenate and Gadoterate did not have enough data for
adequate comparisons.
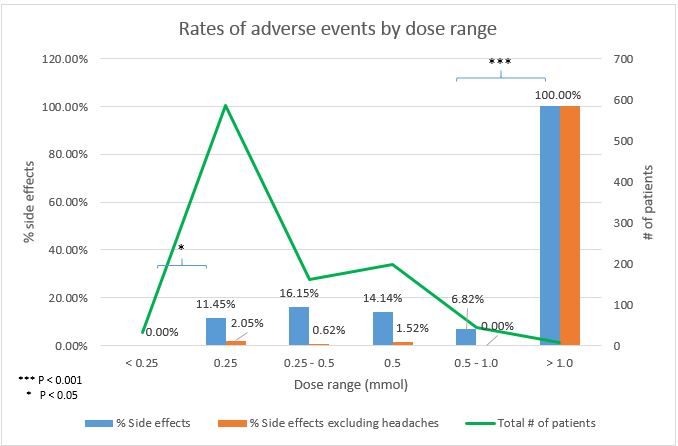
Figure 2. A significant dose x adverse events
relationship exists for GBCAs. Doses below 0.25 mmol have a significantly
lowest risk for overall (blue)
adverse events (zero in our case) than any other dose range. Furthermore, there
is a significant, and potentially life-threatening increase in the rates of
adverse events for GBCA doses beyond 1 mmol. Doses between 0.25 and 1 mmol have
similar rates of adverse events. Note, when transient, postural headaches are
excluded (orange),
the overall rates of adverse events are 2.24%.