1431
An approach to validate MRI Compatible axial Knee joint Loading Device with various standing posture in Standing MRI1Centre of Biomedical Engineering, Indian Institute of Technology Delhi, Delhi, India, 2BME, Amity Uninversity Haryana, ASET, Gurgaon, India, 3Mahajan Imaging Centre, New Delhi, India
Synopsis
Study of knee joint behaviour under load have a significant potential for Osteoarthritis (OA) diagnosis and monitoring. There are few reported studies on monitoring changes in knee cartilage under load using MRI. Reported process of validation of such loading device are in term repeatability and reproducibility. In this study, an approach is proposed to validate the loading-device using MRI data acquired in standing posture. OpenMRI(0.25T) was used to acquire data in various postures and results were compared with 3T-MRI data with and without load reliability and accuracy of various measurements such as bone-gap, cartilage-thickness and T2-values were evaluated.
Introduction
Knee joint loading device has been reported in few studies for understanding the OA progression1,2,3,4,5. In process of validation, repeatability and reproducibility3,4 are important factors. However, there is no reported study on comparison of load distribution using a loading device vs during various standing posture. This comparison is important for validation of loading device and understanding load distribution. Loading of the device behaviour during MRI could not be evaluated directly by any mean rather than standing-MRI. Objective of study is to test weather proposed device is able to generate desire axial load and distribution under 3.0T-MRI. Thus we use 0.25T-Open-Standing-MRI(G-Scan, Estaote) as a tool to compare loading behaviour of proposed loading device with load under various standing postures. This study included bone-gap, cartilage-thickness and T2-values as marker to do comparison.Methods and Materials
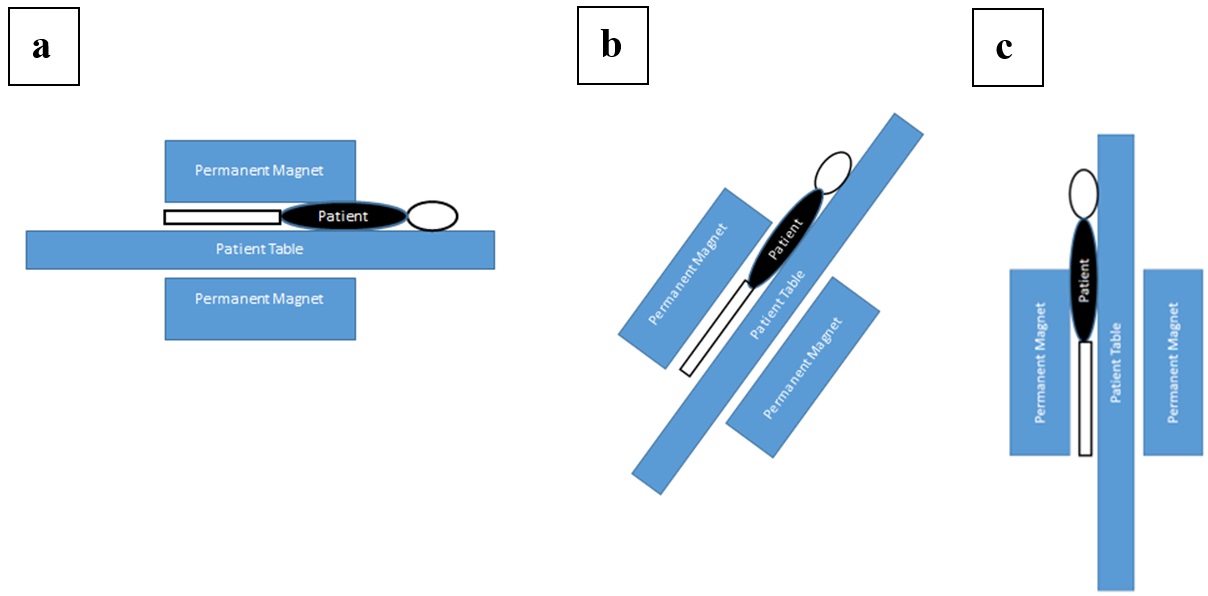
Three healthy volunteers were included in this study, approved by IRB, with prior consent from volunteers. Right leg of each subject was used for MRI data acquisition. A custom built, portable, MRI compatible, knee joint loading device was used during experiment to generate axial load of 50% of body weight on the knee joint. The data set was acquired using two different scanners: 0.25T; 3.0T. Figure-1 show cartoon representing different postures for MRI scanning using 0.25T. Image acquisition with standing MRI included dual PD-T2-weighted. At 3.0T MRI, FS-PD-weighted and T2-mapping(Cartigram) data were acquired.
At 3T MRI, data without and with load using loading device were acquired in supine posture. At 0.25T MRI, data with different posture were acquired: without and with load in supine position; various standing postures as shown in Figure 1a, 1b and 1c. Without load studies, in supine position, were repeated for evaluating reproducibility and robustness of knee joint measures such as bone-gap, cartilage-thickness, T2-values. Experiment protocol is mentioned in Table-1. Bone-gap, cartilage-thickness and cartilage T2-values in lateral and medial compartment of the knee were computed and evaluated for each compartment using in-house developed algorithm. Two investigators segmented the bone gap and cartilage independently. Coefficient-of-variation(CoV) was computed for evaluating reproducibility of various measures.
Results
Table-2 shows values of various measures(bone-gap, cartilage-thickness, T2-values) at 0.25T and 3T, repeated twice. Results are for different subjects and in medial and lateral side. Results show that at 0.25T, only bone-gap is a reliable measure. CoV% for bone-gap at 0.25T was less than 5%. T2 values at 0.25T were obtained using two TE values compared to multi-echo cartigram data at 3T and were quite overestimated compared to actual T2 values of cartilage. COV% for cartilage thickness and T2 values were greater than 5% and therefore these are not a reliable measure to detect loading related changes, which are usually of the same order. On the other hand all three measure are reproducible with COV% under 5%. There was a good agreement between data processing results of two investigators.
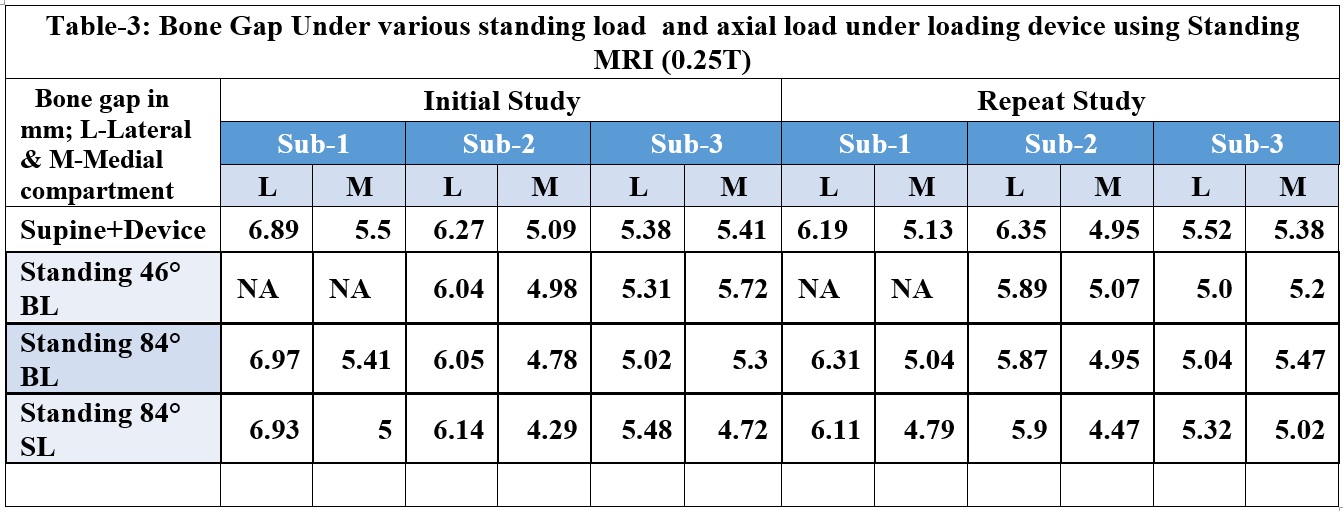
Results of Study-2, are shown in table-3, relative difference of bone-gap in percentage for knee under load with 46° both-legs(BL), 84° both-legs and 84° single-leg(SL) standing postures vs proposed loading device is 4.3%, 3.5% and 6.4%, respectively. The load behaviour of device was observed to be similar to the load behaviour in standing posture at 84° with both legs.
Discussion
Using bone-gap as a measure of load generated on
knee joint, the change in bone-gap while standing on both-leg at 84° was found to be same as the load created by the loading device with 50% body
weight load in the supine posture during MRI scanning. Both these experimental
protocols showed similar results, the CoV was observed to be 3.7% in bone gap
while using loading device at 0.25T and 3.0T. The device also produced
repeatable and reproducible results as was observed with similar bone gap
reduction under 0.25T and 3.0T at different time points. Cartilage thickness
and T2-values could not be calculated at 0.25T because of poor SNR(as shown in figure 2), however
cartilage thickness and T2-values as measure at 3.0T matched with the change in
bone gap under loading conditions. In future the changed in load distribution,
CartiGram and cartilage thickness can be evaluated in four quadrants of the
joint to improve diagnosis and prognosis in OA.
Conclusion
A MRI compatible customized axial loading device for knee joint has been designed. The device is able to simulate load in supine position which is validated as the same as generated in standing position. At 3.0T further studies can now be performed for patients with OA to understand the complex dynamics of knee joint.Acknowledgements
The authors acknowledge the grant support from IRD, IIT Delhi (Project No. MI01422). Authors would also like to thanks Mahajan Imaging Centre, New Delhi for providing the MRI facilities.References
1. R. Patel, Matthew Eltgroth, et al., Loaded versus unloaded magnetic resonance imaging (MRI) of the knee: Effect on meniscus extrusion in healthy volunteers and patients with osteoarthritis, European Journal of Radiology Open 3 (2016) 100–107
2. International application number for patent WO2016100966A1
3. Hongsheng Wang, Matthew F. Koff, et al, An MRI-compatible loading device to assess knee joint cartilage deformation: Effect of preloading and inter-test repeatability, Journal of Biomechanics 48 (2015) 2934–2940
4. Larry Chen, Larry Chen, Karen Gordon and Mark Hurtig, Design and validation of a cadaveric knee joint loading device compatible with magnetic resonance imaging and computed tomography, Medical Engineering & Physics 36 (2014) 1346–1351
5. Westphal, C.J., et al., Load-dependent variations in knee kinematics measured with dynamic MRI. Journal of Biomechanics (2013), dx.doi.org/10.1016/j.jbiomech.2013.05.027
Figures