1429
Scan Time Reduction in High Resolution Knee Imaging using Compressed Sensing and Denoising Deep Learning Reconstruction1Radiology, UCSD, La Jolla, CA, United States, 2Canon Medical Systems Corp., Otawara, Japan, 3VA San Diego Healthcare System, La Jolla, CA, United States
Synopsis
Compressed sensing (CS) uses undersampling at the expense of image blurring and increased noise. We have developed denoising deep learning reconstruction (dDLR) to reduce noise and regain signal-to-noise ratio (SNR) in highly undersampled (4-4.5x) CS images. Feasibility study was performed in fat-suppressed T2 and proton density knee images, by evaluating SNR and image quality (sharpness, blurring, and artifact scores). Compared to reference (no CS or dDLR), images obtained with CS had lower SNR (by 25 to 40%) and image scores due to sharpness and blurring. After processing with dDLR, SNR and image scores were restored the reference levels.
INTRODUCTION
Recently, compressed sensing (CS) has been applied in reduction of scan time in MRI using undersampling1. However, increasing undersampling rate in CS causes image blurring and reduction in signal-to-noise ratio (SNR). Clinical knee imaging includes several protocols with fat suppression that starves SNR. The goal of this feasibility study on knee imaging was to determine performance of denoising deep learning reconstruction (dDLR)2,3 in maintaining image quality, reducing noise and gaining SNR, when CS is used to reduce scan time.Materials and Methods:
Combination of CS and dDLR was applied in 2D FSE knee imaging protocol. CS data collection was applied with variable density Poisson sampling and CS reconstruction was performed with wavelet transformed L1 norm minimization and combining parallel imaging with auto-calibrated map4. In dDLR, multiple images with multiple contrasts were created by adding various levels of noise, and these were used as teaching images. The dDLR noise reduction was performed using deep neural network. Both sagittal T2w and axial PD with fat suppression with and without CS were acquired on healthy volunteers using a clinical 3-T system. Then, dDLR was applied to obtain images. T2 fat-suppressed images were obtained with slice thickness of 2.5 mm, FOV of 16x16 cm, matrix of 416x416, NAQ=1, and a full sampling with a scan time of 5:19 min and CSx4.5 times of 1:14 min. The axial PD fat-suppressed images were obtained with slice thickness of 3.0 mm, FOV of 16x16 cm, matrix of 448x448, NAQ=1, and a full sampling with a scan time of 5:21 min and CSx4 times of 1:24 min. Various regularization factors, r (λ=10r-4), of 1.4, 2.0, and 2.5 were applied in CS, followed by dDLR processing. SNRs of bone, muscle, and fluid were measured, and compared against SNRs from the reference images (i.e., full-sampling without CS or dDLR) as ratios. We also evaluated image quality semi-quantitatively for sharpness, blurring, artifacts, and overall image quality using a 4-point scale (0; poor, 1; fair, 2; good, and 3; excellent).Results:
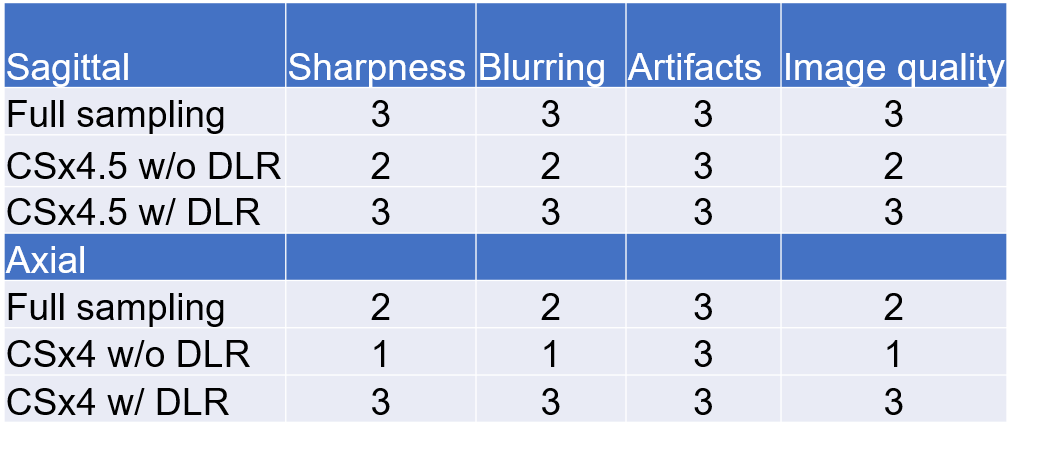
Both sagittal T2 (Figure 1A) and axial PD (Figure 1D) fat-suppressed images showed notable reduction in SNR and image quality with CS (Figure 1B,E), which were recovered after applying dDLR (Figure 1C,F). In different tissues of the knee, SNR ratios are shown in Table 1. On average, the application of CS reduced SNR to around 0.67 as compared to the full sampling; however, dDLR regained the SNR to 1.3 that is about 30 % more signal than the full sampling. The visualization scores as shown in Table 2. In the evaluation of regularization factors, r =1.4 was noisy, r =2.5 was blurred, and r=2.0 appeared optimal with less blurring and sufficient SNR in both T2 and PD images. With application of dDLR, image quality was maintained using the CS reduction factors of 4.5 times in the sagittal T2 images and 4.0 times in the axial PD.Discussions and Conclusion:
Combination of CS and dDLR allows tremendous reduction of scan time in T2 and PD FSE with fat suppression with maintaining good SNR knee imaging. In term of image quality, application of dDLR in high CS reduction imaging permits similar image as the reference image. It remains to be established if dDLR processing affect diagnostic performance. Optimization of dDLR parameters for both speed and diagnosis will requires a larger study with additional teaching images and cases.Acknowledgements
No acknowledgement found.References
1] Lustig M, Donoho D, Pauly JM. Magn Reson Med 2007; 58: 1182-1195.
2] Isogawa K, Ida T, Shiodera T, and Takeguchi T. IEEE Signal Processing Letters 2018;25,224-228.
3] Shinoda K, Isogawa K, Nambu M, et al. ISMRM 2019 submitted.
4] Uecker M, et al., Magn Reson Med 2014; 71: 990-1001.
Figures