1427
A Prospective, Longitudinal Assessment of Adverse Local Tissue Reactions in Resurfacing Hip Arthroplasty Versus Primary Total Hip Arthroplasty in Asymptomatic Subjects1Hospital for Special Surgery, New York, NY, United States
Synopsis
This prospective study compares the prevalence of MRI detected adverse local tissue reactions (ALTRs) in metal-on-polyethylene (MoP), metal-on-metal hip resurfacing arthroplasty (HRA), and ceramic-on-polyethylene (CoP) total hip arthroplasty subjects. Images acquired at four time points with a 1-year interval showed a higher prevalence of ALTRs in the HRA than CoP or MoP subjects. Self-assessed symptomatology scores did not significantly differ by implant type at follow-up, indicating that ATLRs can be clinically silent. This study permits better understanding of the natural history of ALTRs complicating hip arthroplasty.
Introduction
The scientific interest in the development of adverse local tissue reactions (ALTRs) near total hip replacements (THRs) has been recently been revived due to recalled metal-on-metal (MOM) THRs and hip resurfacing arthroplasty (HRA) [1,2]. Notably, ALTRs have also been attributed to corrosion and wear generation at the head/neck junction in traditional implant designs including ceramic-on-polyethylene (CoP) or metal-on-polyethylene (MoP) [3,4]. Failure of MOM THRs and HRAs due to development of adverse local tissue reaction (ALTRs) is associated with high morbidity [5]. The purpose of this prospective longitudinal study was to: 1) determine ALTR prevalence in asymptomatic patients with different types of HRA, MoP, and CoP implants; 2) determine if patients with HRA have a greater rate of ALTRs compared to patients with CoP and MoP THA; and 3) evaluate changes in patient reported outcomes in these three types of implant designs. We hypothesized that patients with HRA would have similar self-assessed joint function to CoP and MoP subjects but also have a greater prevalence of ALTRs on MRI.Methods
Following IRB approval with informed consent, primary CoP, MoP and HRA patients more than one year post-arthroplasty were evaluated with annual MRIs using clinical 1.5T scanners (GE Healthcare, Waukesha, WI) and 8 channel cardiac coils (Invivo, Gainesville, FL). Morphologic and susceptibility reduced images were acquired [6,7] and evaluated for the presence of synovitis, synovial thickness and volume, and the presence of MRI ALTR [8,9]. Patient reported outcomes were evaluated by Hip Disability and Osteoarthritis Outcome Scores (HOOS)[10]. Statistical analysis included: 1) mixed-effects modeling to compare synovial thickness, synovial volume, and HOOS subgroups between bearing surfaces at each time point and within each bearing surface over time and 2) Cox proportional hazards modeling to compare the time to and the risk of developing ALTR between bearing surfaces. All models were adjusted for age, gender, and length of implantation. Significance is set at p<0.05. (SAS v9.4, Cary, NC).Results
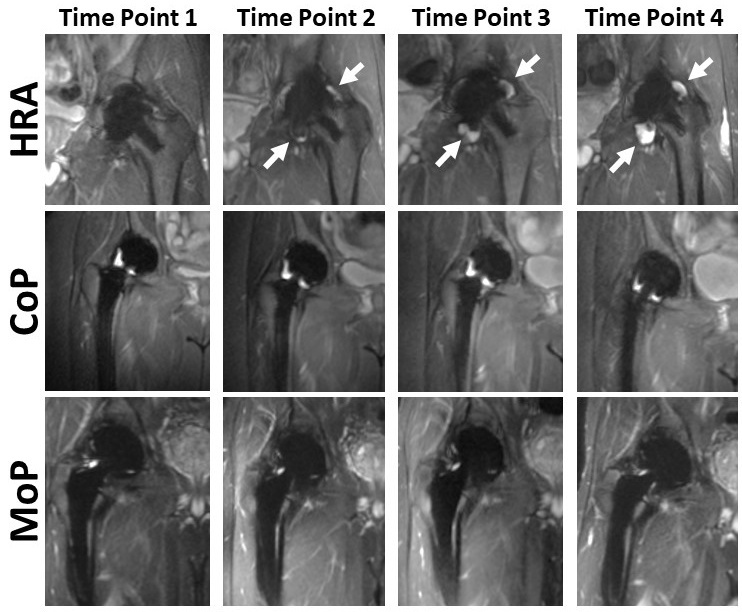
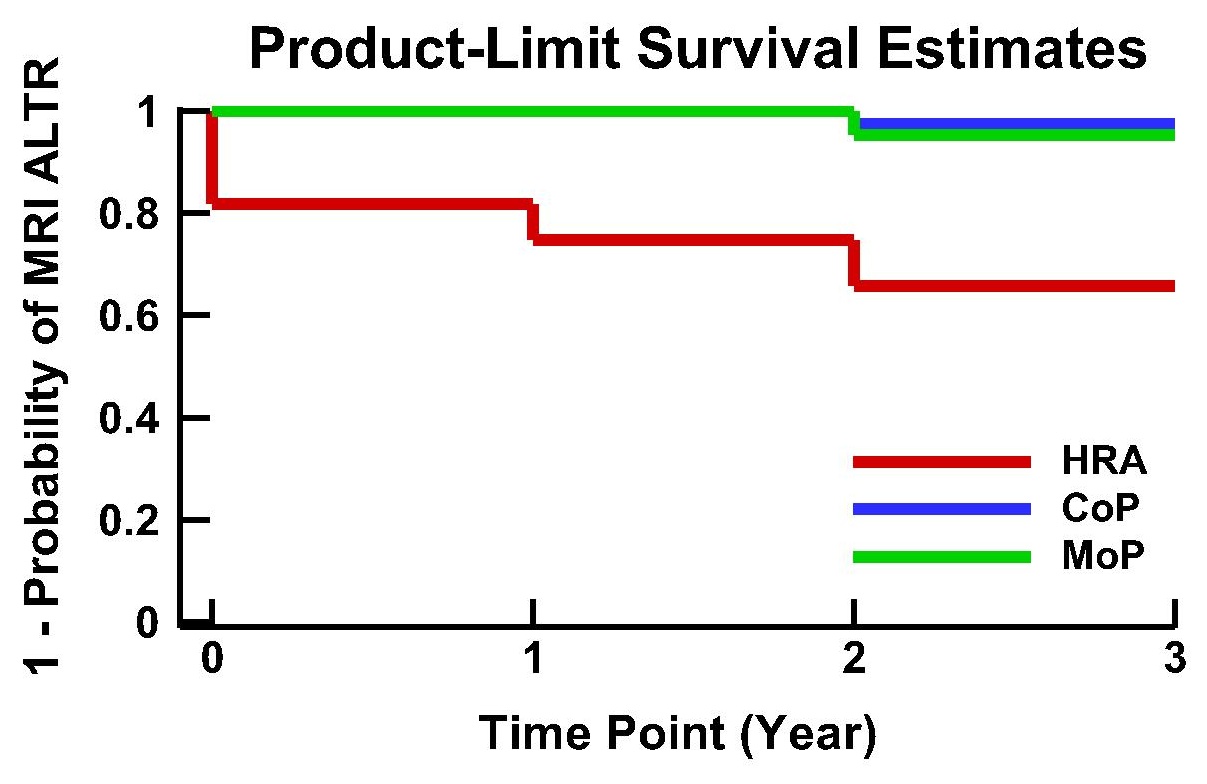
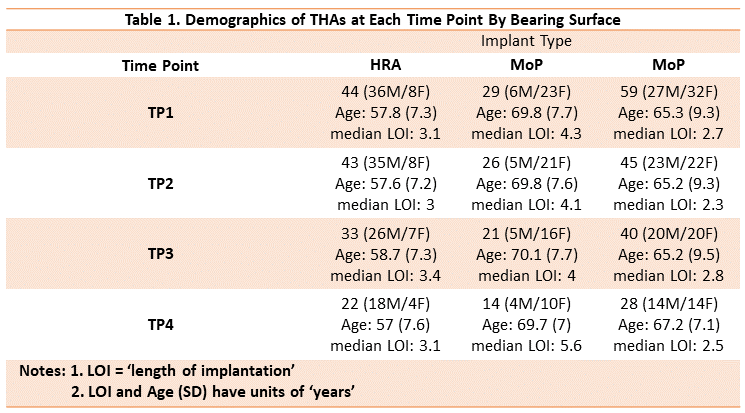
132 hips (128 subjects) were evaluated at the initial time point (TP1). Subject demographics and length of implantation (LOI) by bearing surface is displayed in Table 1. The mean synovial thickness of HRA was greater than MoP (mean diff.=0.8±0.3mm, p=0.01) only at TP1 (HRA: 2.8±0.2mm; MoP: 2±0.2mm), while HRA synovial thickness was greater than CoP at TP1 (CoP: 2.3±0.2mm; mean diff=0.5±0.2mm, p=0.04) and at TP2 (HRA: 2.5±0.2mm; CoP: 1.9±0.2mm; mean diff=0.6±0.3mm, p=0.03). The mean synovial volume of the HRA, MoP, and CoP subjects was similar at TP1 (HRA: 5±3cm3; MoP: 3±4cm3; CoP: 5±2cm3, p=0.9). The mean synovial volume in HRA subjects increased from TP1 to TP4 (mean vol. diff=+7.7±3.2cm3, p=0.02), while CoP subjects and MoP subjects only displayed a slight change in synovial volume (CoP: mean vol. diff=-0.5±2.8cm3, p=0.96; MOP: mean vol. diff=-1.1±9.3cm3, p=0.9, Figure 1). The synovial volume in HRA subjects was larger than CoP and MoP subjects at TP4 (HRA: 12±3.7cm3; CoP: 5±3cm3; MoP: 1±4cm3), but the differences were not significant (MOP: p=0.07; CoP: p=0.1). By TP4, 14 cases of ALTRs developed in the HRA subjects (mean time to ALTR=1.6 yrs.), as compared to 1 case in the CoP (mean time to ALTR=2 yrs.) and 1 case in MoP subjects (mean time to ALTR=2 yrs.) (Figure 2). The risk of ALTRs in HRA subjects is 24 times (95% CI: 3-211, p<0.01) the risk in CoP subjects. The risk of ALTRs in MoP subjects is 1.6 times (95%CI:0.1 to 26.8, p=0.8) the risk in CoP subjects. The HOOS scores of HRA subjects were similar to CoP and MoP subjects from TP1 to TP4 in subcategories of Pain, Symptoms, Activities of Daily Living, and Quality of Life. However, HRA subjects had better scores in the ‘Sporting’ subcategory than CoP and MoP subjects at each time point (mean diff. range: +8.6 to +13.2, p<0.05).Discussion/Conclusion
This prospective, longitudinal study found an increase of synovial volume and significantly higher rate of ALTRs in the HRA subjects even as patient self-assessed symptomatology of HRA subjects was similar or better than CoP and MoP subjects. These findings indicate that MRI detected ALTRs in high functioning subjects without complaints of pain; thus an annual clinical assessment that is dependent upon symptoms alone may not detect patients with soft tissue complications until extensive soft tissue damage occurs and affects joint function. MRI is a non-invasive imaging modality that is uniquely capable of assessing peri-prosthetic soft tissue complications and should be considered part of the routine follow up for this patient population to allow for early detection and monitoring of ALTRs.Acknowledgements
Research reported in this publication was supported by NIH/NIAMS R01AR064840. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.References
1. Hart AJ, Sabah S, Henckel J, Lewis A, Cobb J, Sampson B, Mitchell A, Skinner JA. The painful metal-on-metal hip resurfacing. J Bone Joint Surg Br. 2009;91:738-744.
2. Kwon YM, Ostlere SJ, McLardy-Smith P, Athanasou NA, Gill HS, Murray DW. "Asymptomatic" pseudotumors after metal-on-metal hip resurfacing arthroplasty: prevalence and metal ion study. J Arthroplasty. 2011;26:511-518.
3. Walsh AJ, Nikolaou VS, Antoniou J. Inflammatory pseudotumor complicating metal-on-highly cross-linked polyethylene total hip arthroplasty. J Arthroplasty. 2012;27:324 e325-328.
4. Carli A, Reuven A, Zukor DJ, Antoniou J. Adverse soft-tissue reactions around non-metal-on-metal total hip arthroplasty - a systematic review of the literature. Bull NYU Hosp Jt Dis. 2011;69 Suppl 1:S47-51.
5. Laaksonen I, Donahue GS, Madanat R, Makela KT, Malchau H. Outcomes of the Recalled Articular Surface Replacement Metal-on-Metal Hip Implant System: A Systematic Review. J Arthroplasty. 2017;32:341-346.
6. Koch KM, Lorbiecki JE, Hinks RS, King KF. A multispectral three-dimensional acquisition technique for imaging near metal implants. Magn Reson Med. 2009;61:381-390.
7. Potter HG, Nestor BJ, Sofka CM, Ho ST, Peters LE, Salvati EA. Magnetic resonance imaging after total hip arthroplasty: evaluation of periprosthetic soft tissue. J Bone Joint Surg Am. 2004;86-A:1947-1954.
8. Nawabi DH, Hayter CL, Su EP, Koff MF, Perino G, Gold SL, Koch KM, Potter HG. MRI Findings in Symptomatic vs. Asymptomatic Subjects Following MOM Hip Resurfacing Arthroplasty. J Bone Joint Surg Am. 2013;95:895-902.
9. Nawabi DH, Gold S, Lyman S, Fields K, Padgett DE, Potter HG. MRI predicts ALVAL and tissue damage in MOM hip arthroplasty. Clin Orthop Relat Res. 2014;472:471-481.
10. Nilsdotter AK, Lohmander LS, Klassbo M, Roos EM. Hip disability and osteoarthritis outcome score (HOOS)--validity and responsiveness in total hip replacement. BMC Musculoskelet Disord. 2003;4:10.
Figures