1412
Usefulness of Magnetic Resonance Texture Analysis for Differentiation between Recurrent Disc Herniation and Postoperative Epidural Fibrosis1Department of Radiology, Kyung Hee University Hospital at Gangdong, Seoul, Korea, Republic of, 2Department of Radiology, Kyung Hee University Hospital, Seoul, Korea, Republic of
Synopsis
Although magnetic resonance (MR) with
contrast-enhancement has been used as standard imaging tool for distinguishing
recurrent disc herniation from postoperative epidural fibrosis, it is
relatively invasive and vulnerable to contrast material-related complication. Also,
the differentiation between recurrent disc herniation and postoperative
epidural fibrosis on non-enhanced MR is not always clear. Until now, no study
has evaluated the diagnostic usefulness of MR texture analysis (MRTA) for
differentiation between recurrent disc herniation from postoperative epidural
fibrosis. Therefore, the purpose of this study is to evaluate the usefulness of
MRTA for differentiation between recurrent disc herniation from postoperative
epidural fibrosis. Regarding mean, skewness, MPP, and entropy, values on all
sequences were significantly lower in recurrent disc herniation than those in
postoperative epidural fibrosis (p<0.001).
The best performing MRTA parameters were MPP on T2WI (AUC, 0.81; 95 % CI, 0.72-0.90)
and on T1WI (AUC, 0.80; 95 % CI, 0.70- 0.88). There were excellent
interobserver agreements for all measurements (ICC, 0.838–0.905).
Introduction
The diagnostic evaluation of patients presenting with failed back surgery syndrome is a challenge to both radiologists and surgeons. Although the cause of this syndrome is complex and often multifactorial, recurrent disc herniation and postoperative epidural fibrosis at the previously explored level(s) are frequent sources of symptoms (1). On non-enhanced magnetic resonance (MR) imaging, the discrimination between recurrent disc herniation and postoperative epidural fibrosis is not always clear because of overlapping imaging features. Although MR with contrast-enhancement has been used as standard imaging tool for distinguishing recurrent disc herniation from postoperative epidural fibrosis (2, 3), it is relatively invasive and vulnerable to contrast material-related complication. Therefore, a needs exists the non-invasive, advanced, less subjective imaging method that could help distinguish recurrent disc herniation from postoperative epidural fibrosis. Recently, texture analysis (TA) is a advanced image analysis technique that can detect and quantify heterogeneity of tissue characteristics which cannot be detected by the human eye (4, 5). To our best knowledge, no study has evaluated the diagnostic usefulness of MRTA for distinguishing recurrent disc herniation from postoperative epidural fibrosis. Therefore, the purpose of this study is to evaluate the usefulness of MRTA for differentiation recurrent disc herniation and postoperative epidural fibrosis.Methods
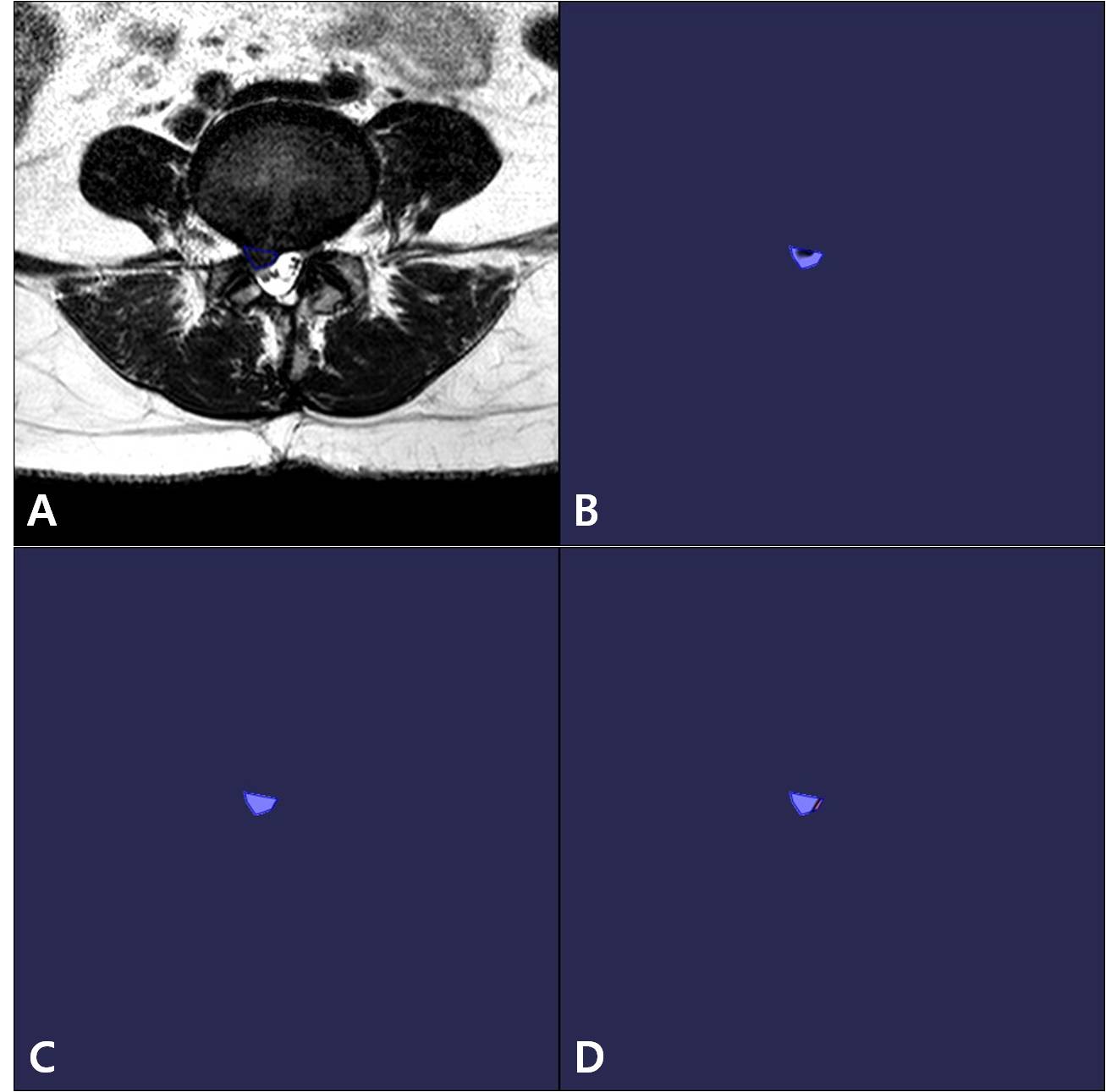
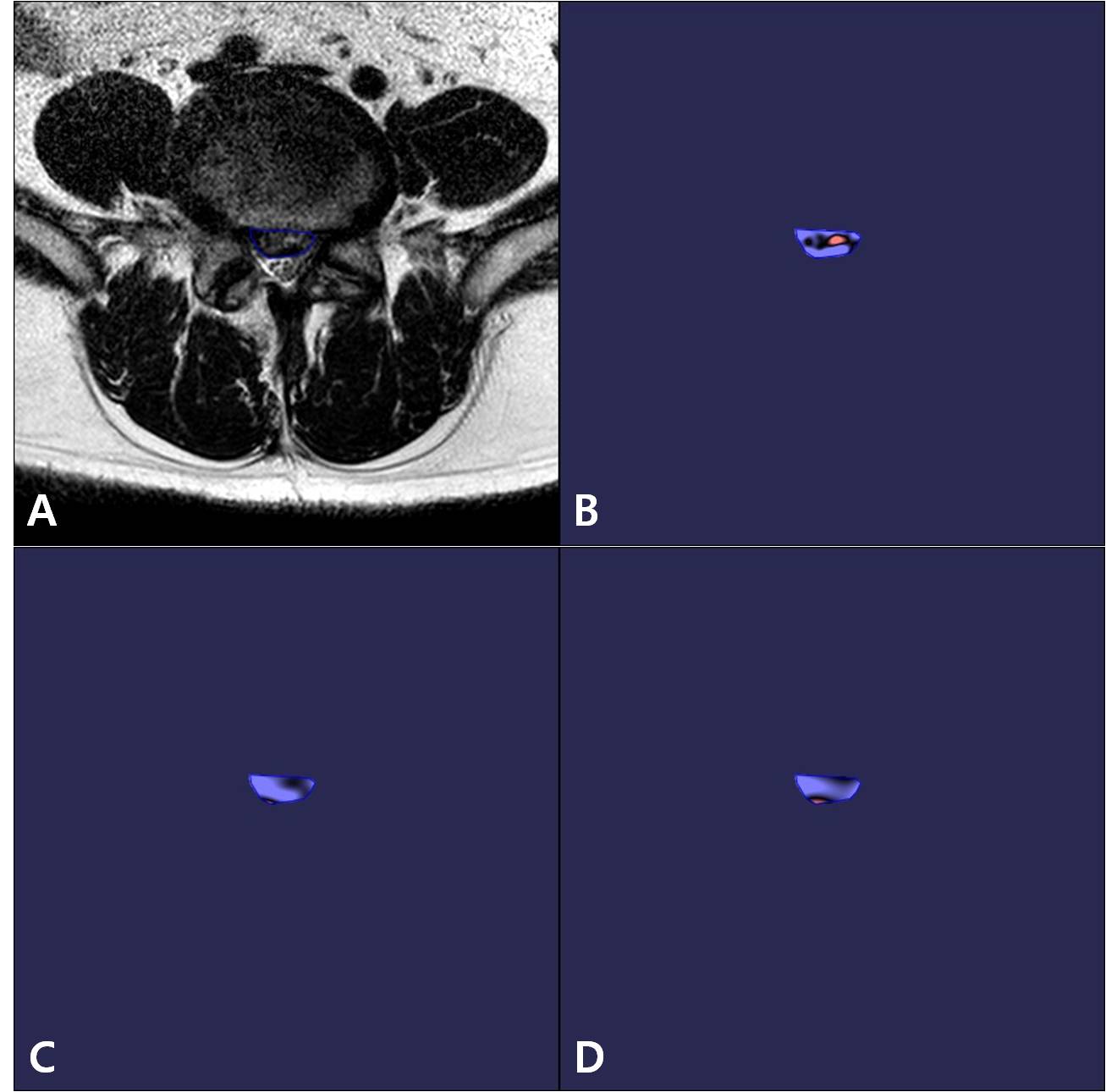
From December 2006 to April 2018, a total of 72 consecutive patients with recurrent disc herniation (n=50) and postoperative epidural fibrosis (n=22) were initially included. Among them, three patients were excluded because of the metallic artifact (n=2) and severe motion artifact (n=1). MRI was obtained using a 3-T system or 1.5-T system. The MRI protocols included axial and sagittal T2-weighted fast spin-echo (T2WI), sagittal T2-weighted fast spin-echo with fat suppression image (T2FS), axial and sagittal T1-weighted image (T1WI), and axial and sagittal T1-contrast-enhanced (T1CE) images. Recurrent disc herniation was confirmed by surgical finding. And postoperative epidural fibrosis was confirmed by clinical follow-up at least 6 months (symptoms relieved via only conservative treatment). Axial T2WI and axial T1WI were uploaded into proprietary TexRAD research software. Region of interests (ROIs) were drawn independently by two reviewers with a 1-week interval. Reviewers were blinded to any patients’ information. For ROI placement, “seedpoint” mode was used which was automatically drawing ROI along the margin of the mass by click the mass. If the automatically drawn ROI was located in outside of the mass, it was permitted that the reviewer modified the ROI freehand with “polygonal” mode. The ROIs were automatically drawn in all axial images in which the mass was included and summed the information from the each ROIs using “batch” reconstruction. Regarding the order of the MR sequence, all ROIs were initially drawn on the axial T2WI. And then, ROIs was copied and placed for axial T1WI. Quantification of histograms was based on mean, skewness, mean of positive pixels (MPP), kurtosis, and entropy. Statstically, the independent t-test, receiver operating characteristic (ROC) curve, and intraclass correlation coefficient (ICC) were performed.Results
A total of 69 patients (mean age 45.7±12.6 years; range), including 36 male (mean age 48.2±15.5 years; range 35-72) and 33 female (mean age 43.4±12.6 years; range 38-67), were ultimately enrolled in this study. Regarding mean, skewness, MPP, and entropy, values on all sequences were significantly lower in recurrent disc herniation than those in postoperative epidural fibrosis (p<0.001). However, regarding kurtosis, values on all sequences were not different between recurrent disc herniation and postoperative epidural fibrosis (p=0.39-0.68). The best performing MRTA parameters were MPP on T2WI (AUC, 0.81; 95 % CI, 0.72-0.90) and on T1WI (AUC, 0.80; 95 % CI, 0.70- 0.88). There were excellent interobserver agreements for all measurements (ICC, 0.838–0.905).Conclusion
In conclusion, texture metrics in MRTA parameters were different between recurrent disc herniation and postoperative epidural fibrosis. Among them, MPP on T2WI and T1WI were most useful for differentiating recurrent disc herniation and postoperative epidural fibrosis. Therefore, MRTA shows promise as a tool for differentiation between recurrent disc herniation and postoperative epidural fibrosis without use of the MR contrast material.Acknowledgements
None.References
1. Burton CV. Causes of failure of surgery on the lumbar spine: ten-year follow-up. Mt Sinai J Med. 1991;58(2):183-187.
2. Bundschuh CV, Modic MT, Ross JS, Masaryk TJ, Bohlman H. Epidural fibrosis and recurrent disk herniation in the lumbar spine: MR imaging assessment. AJR Am J Roentgenol. 1988;150(4):923-932.
3. Sotiropoulos S, Chafetz NI, Lang P, et al. Differentiation between postoperative scar and recurrent disk herniation: prospective comparison of MR, CT, and contrast-enhanced CT. AJNR Am J Neuroradiol. 1989;10(3):639-643.
4. Ganeshan B, Miles KA. Quantifying tumour heterogeneity with CT. Cancer Imaging. 2013;13:140-149.
5. Miles KA, Ganeshan B, Hayball MP. CT texture analysis using the filtration-histogram method: what do the measurements mean? Cancer Imaging. 2013;13(3):400-406.
Figures