1409
Clinical shoulder MR imaging at 7 Tesla in comparison to arthroscopy and 1.5 Tesla MRI1Erwin L. Hahn Institute for MRI, University Duisburg-Essen, Essen, Germany, 2Department of Diagnostic and Interventional Radiology and Neuroradiology, University Hospital Essen, Essen, Germany, 3High Field and Hybrid MR Imaging, University Hospital Essen, Essen, Germany, 4Department of Trauma and Orthopedic Surgery, University Hospital Essen, Essen, Germany, 5Facharztklinik Essen, Essen, Germany
Synopsis
An 8-channel transmit/15-channel receive radiofrequency coil setup for 7T shoulder imaging has been evaluated in eight patients presenting with shoulder pain. In total, ten gradient echo and turbo spin echo sequences were included in the imaging protocol. Image quality was assessed in consensus by two radiologists. A structured report focusing on the rotator cuff was generated based on the 7T images and subsequently compared with the arthroscopical report taken as the gold standard. Finally, pathologies found at 7T were visually compared with preexisting 1.5T MR images from the same patients.
INTRODUCTION
While the FDA has already cleared MR imaging of the knee joint at 7T as a clinical application for the latest generation of 7T MR systems [1], MRI of the shoulder at 7T is still in its infancy. A recent publication introduced a two-array RF coil setup for shoulder imaging featuring an 8-channel transmit/receive coil based on microstrip lines with meanders and a 7-channel receive-only coil based on loops [2]. Anatomical images in healthy volunteers demonstrated the high performance of the RF coil setup to acquire high-resolution 7T shoulder imaging with excellent image quality. In this work, the RF coil setup will be further evaluated in a patient cohort.METHODS
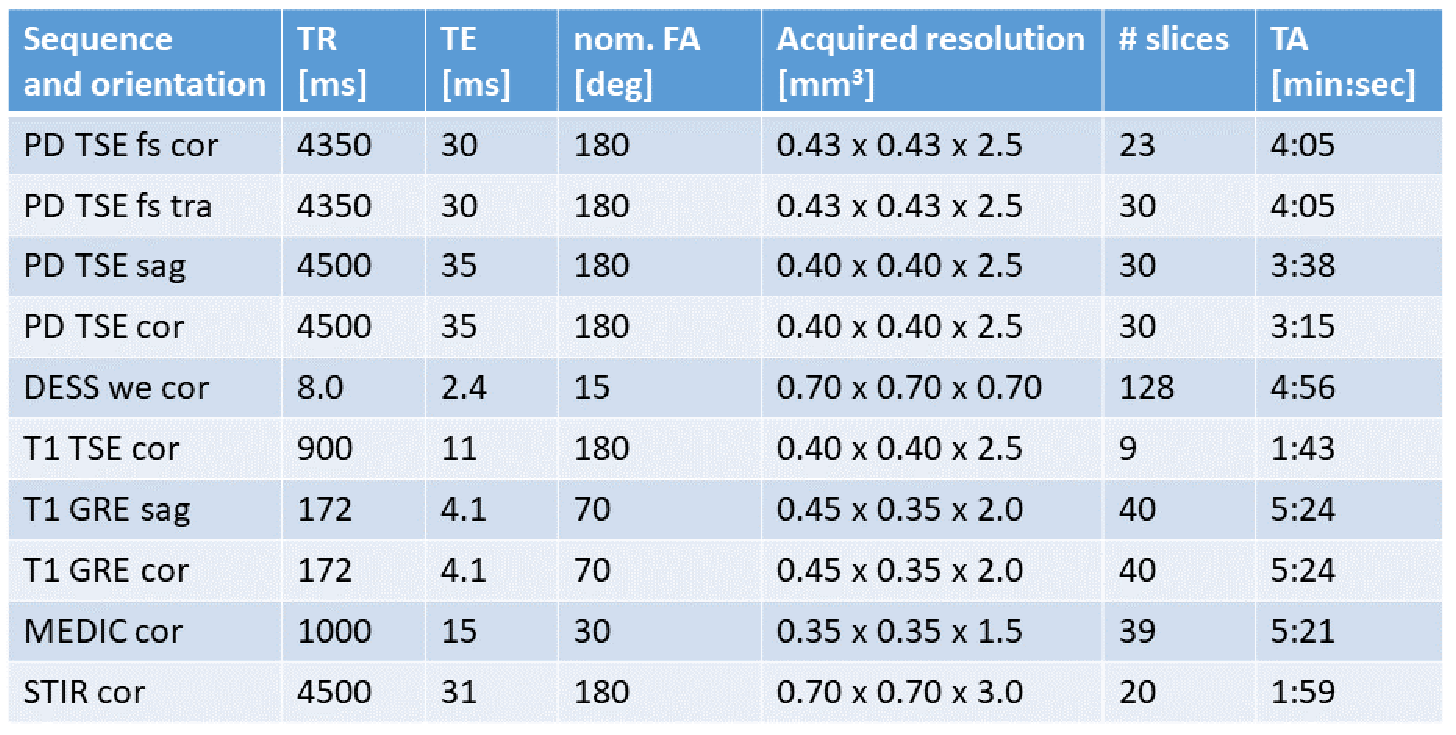
In cooperation with a surgeon, eight patients (6 male, 2 female; 48.3 ± 10.0 years) presenting with shoulder pain and being scheduled for arthroscopic surgery of the affected shoulder in the orthopedic outpatient department participated in the study and signed informed consent. A whole-body research system (Magnetom 7T, Siemens Healthcare, Germany) equipped with the above mentioned RF coil setup was used for imaging [2]. To minimize B1+ inhomogenities while obtaining maximum signal amplitude, phase-only RF shimming was used. In total, ten optimized sequences were included in the protocol, balancing a maximum of variety for evaluation and short examination time. Details about the sequence parameters are provided in Figure 1. Image quality was assessed in consensus by two radiologists separately for each patient and each sequence. Therefore, the presence of artifacts was rated on a 5-point scale, the impact of B1+ inhomogenities on a 3-point scale and the delineation of anatomical structures on a 4-point scale. The higher the rating, the better the image quality. Additionally, a structured report focusing on the rotator cuff was generated in consensus by the same radiologists, assessing fatty atrophy of the rotator cuff muscles, supraspinatus atrophy, the subacromial subdeltoideal bursa, lesions of the tendons, degeneration of acromioclavicular (AC) joint, effusion of the glenohumeral joint, as well as the status of the cartilage, and the labrum. The outcome of the report was afterwards compared with the arthroscopical report taken as the gold standard. Finally, pathologies found at 7T were visually compared with preexisting 1.5T MR images from the same patients.RESULTS
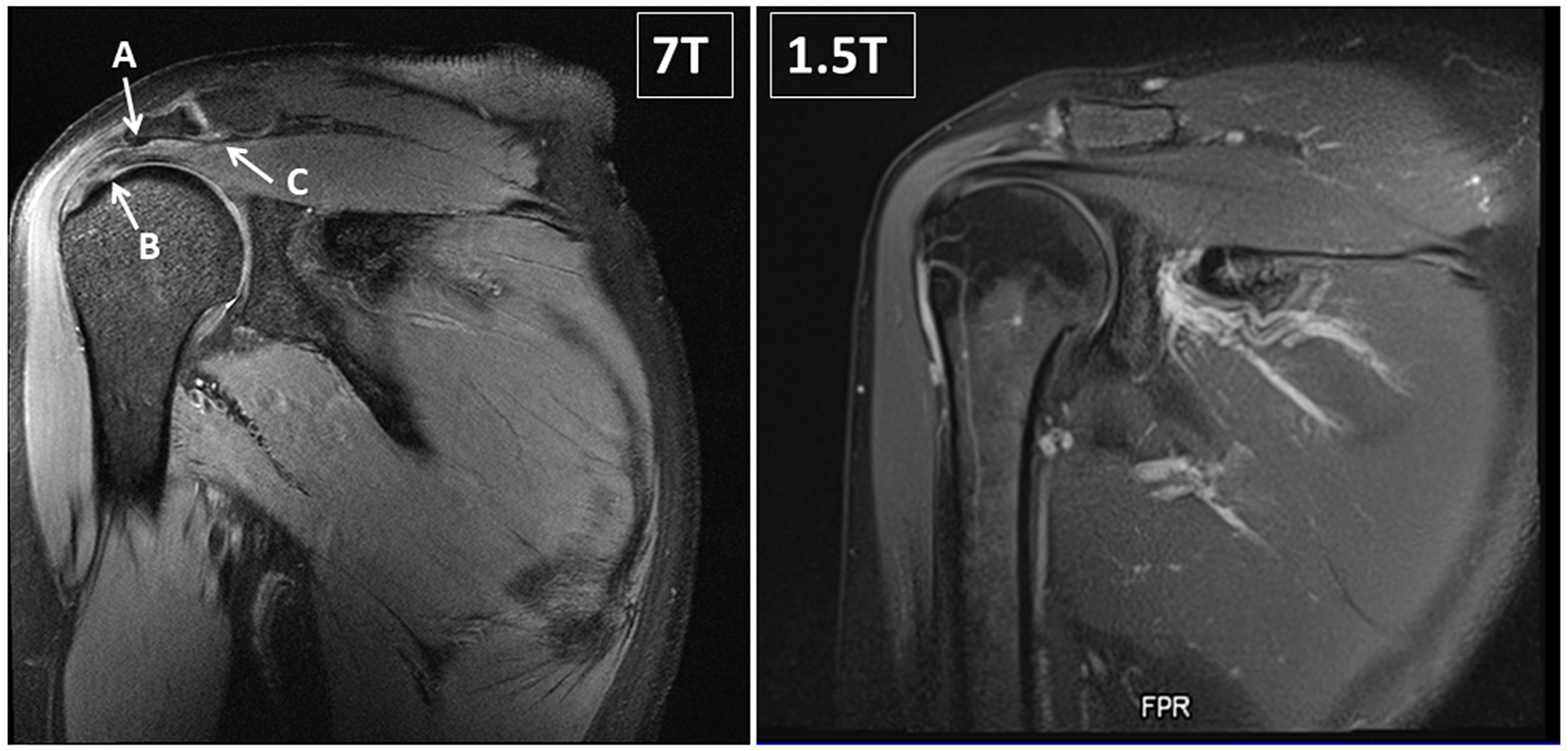
Very good image quality with hardly definable artifacts was observed in PD TSE fs, while moderate artifacts appeared in MEDIC and STIR sequences. The most homogenous B1+ field was observed in T1 GRE and DESS. Strongest inhomogeneities appeared in MEDIC cor and PD TSE sag. Likewise, with the exception of vessels and nerves, the delineation of anatomic structures was best in PD TSE fs and impaired in MEDIC and STIR. For vessels and nerves PD TSE cor and T1 GRE were rated best, while fat saturated PD TSE sequences underperformed. For the evaluation of muscle tissue, DESS and T1 GRE could complement PD TSE fs sequences. Details are shown in Figure 2. Pathologies of the rotator cuff were identified at 7T in every patient. In correlation with the arthroscopical report (delay between 7T MRI and arthroscopy was 2 – 15 days in 7 patients, and 70 days in 1 patient) pathologies of the rotator cuff tendons were widely overdiagnosed with 7T MRI: With arthroscopy, tendinitis or partial tear of the supraspinatus tendon was confirmed in only 3 of 8 patients, of the infraspinatus tendon in 0 of 1 patient and of the subscapularis tendon in 1 of 6 patients. According to arthroscopy, only one pathology of the rotator cuff (partial lesion of the subscapularis tendon) was missed with 7T MRI. Pathologies of the long bicipital tendon, the AC-joint, the glenohumeral cartilage, the labrum and the subacromial subdeltoideal bursa were mainly concordant in arthroscopy and 7T MRI. Exceptions were one lesion of the long bicipital tendon, one subacromial bursitis and one SLAP-lesion missed at 7T (Figure 3). Preexisting 1.5T MRI images could be collected from three patients. The delay between the two examinations was 34, 34 and 49 days, respectively. The main pathologies were visible at both field strengths. However, at 7T pathologies were more distinct due to better contrast and higher image resolution (Figures 4/5).DISCUSSION
Feasibility of clinical 7T MRI of the shoulder was demonstrated. A comprehensive protocol should include fat saturated PD TSE sequences (excellent delineation of almost all anatomical structures) in axial and coronal orientation and a DESS sequence (isotropic high resolution and muscle delineation). A T1 GRE may complement the protocol for its good depiction of vessels and nerves, while the use of STIR needs to be postponed until substantial optimization yields better results. This comprehensive protocol results in a clinically relevant total acquisition time of 25 minutes.Acknowledgements
No acknowledgement found.References
[1] https://usa.healthcare.siemens.com/news/magnetomterrafdaclearance.html, accessed 2018, Oct 5th
[2] Rietsch SHG, et al., An 8-channel transceiver 7-channel receive RF coil setup for high SNR ultrahigh-field MRI of the shoulder at 7T, Med Phys. 2017 Dec;44(12):6195-6208.
Figures