1388
The role of contrast-enhanced whole-body joint MRI in juvenile idiopathic arthritis (JIA)1Faculty of Health Sciences, Hokkaido University, Sapporo, Japan
Synopsis
Due to the limitations of clinical description in diagnosis of juvenile idiopathic arthritis(JIA) with subjective factors, this study attempts to explore the role of contrast-enhanced whole-body MRI(WBMRI) in the JIA. We evaluated the WBMRI images of 156 joint regions of 7 patients, including image quality and positive findings, and compared the results with clinical descriptions. The results showed that WBMRI could observe the lesion of joints more objectively and comprehensively than the clinical description, and could show the changes of the lesions with treatment. Therefore, WBMRI may be used to help diagnose JIA and to evaluate the therapeutic effect.
Introduction
Nowadays, the assessment of affected joints in juvenile idiopathic arthritis (JIA) depend mainly on clinical description1, which is limited by its subjective nature. Besides, the patient may be too young to communicate. All of these can affect the early and accurate diagnosis of JIA. Previous studies of imaging examinations tended to focus on limited anatomical regions such as sacroiliac joints and hips as well as wrists, hands, and feet. 2-4 Therefore, the purpose of this study was to assess the role of contrast-enhanced whole-body joint MRI (WBMRI) in detecting juvenile idiopathic arthritis (JIA) lesions comparing with clinical description.Methods
In this study, 7 pediatric patients (6 females; median age / age range, 11 / 3–16 years) with 12 MR sessions (5, 1, and 1 patients had 1, 3, and 4 MR studies, respectively) were analyzed. MR images were evaluated by a radiologist, which were compared with clinical descriptions. Evaluation included image quality, positive findings such as synovial enhancement and soft tissue swelling.Results
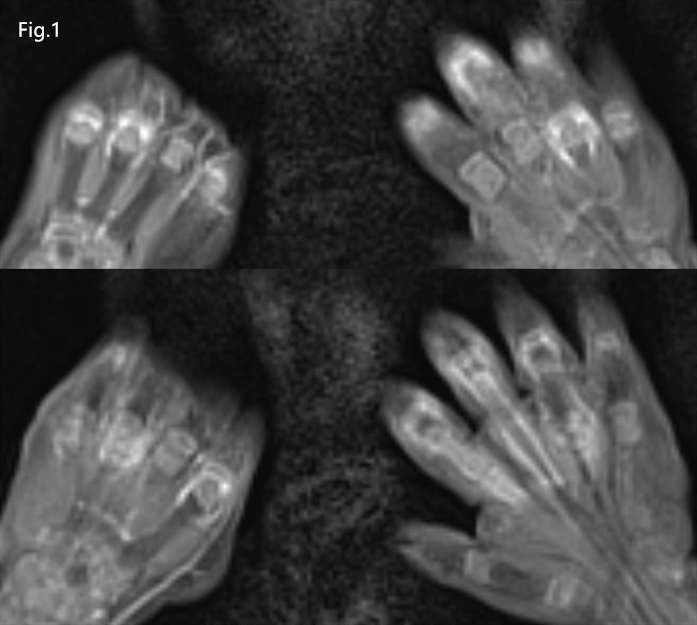
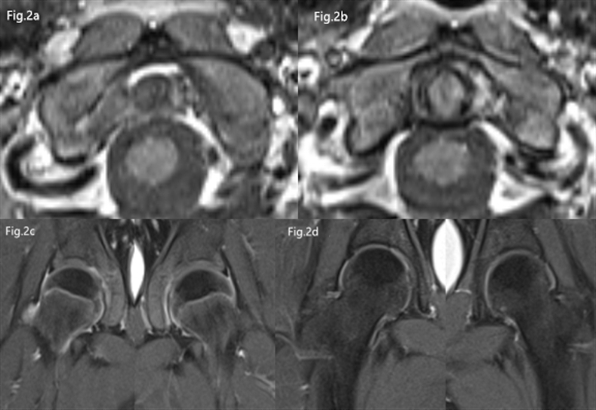
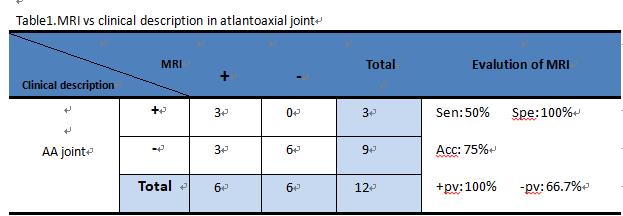
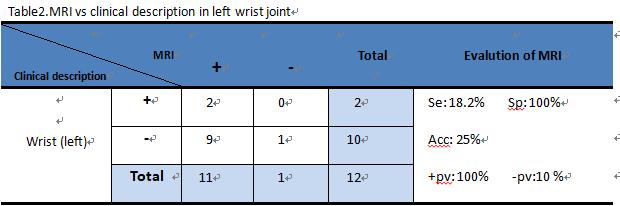
156 regions were evaluated (12 MR sessions with 13 regions for every MR session). The image quality of atlantoaxial regions, hand regions, hip regions was excellent grade in all sessions (100%); that of shoulder regions was excellent grade in 10 sessions (83.3%) and good in 2 sessions (16.7%), that of knee regions was excellent grade in 9 sessions (75%) and good grade in 3 sessions (25%); and that of foot regions was excellent grade in 6 sessions (50%) and good grade in 6 sessions (50%). If we set positive findings as gold standard, the evaluation ability of clinical description in JIA patients was as follows: sensitivity 31.7%, specificity 83.8%, accuracy 54.6%, positive predictive value 68.2%, negative predictive value 52.5%.Discussion
All of the image quality of WBMRI images shows excellent or good level due to the anesthetic effect on pediatric patients, which reduced the movement of children who could not remain stationary for a long time and thus reduced the generation of artifacts. When we assume WBMRI has a high sensitivity to JIA, clinicians only describe the main symptoms and some clinical positive symptoms are not expressed by patients. Therefore, WBMRI can make up for the shortcoming evaluated by the clinical examination for JIA, allowing contrast agent to gather and develop in the lesion site through the increased capillary permeability at the synovial membrane of the pathological joint, and then objectively observed some abnormal regions not described by the clinicians or not expressed by the patients. Moreover, for patients receiving long-term treatment, regular WBMRI examination can more simply observe the changes in the joints of each part of the patient relative to the previous examination, so as to adjust the treatment regimen according to the changes.Conclusion
For pediatric patients suspected of JIA, WBMRI can be obtained with acceptable quality. At the same time, WBMRI is highly sensitive to the detection of JIA, and makes up for the limited clinical assessment resulting from subjectivity for both physician and patient sides. Therefore, WBMRI may be useful to help diagnose JIA and evaluate disease evolution and therapeutic effect.Acknowledgements
No acknowledgement found.References
1. Nusman, C.M., et al., Imaging in juvenile idiopathic arthritis — international initiatives and ongoing work. Pediatric Radiology, 2018. 48(6): p. 828-834.
2. Marteau, P., et al., Conventional radiography in juvenile idiopathic arthritis: Joint recommendations from the French societies for rheumatology, radiology and paediatric rheumatology. European Radiology, 2018. 28(9): p. 3963-3976.
3. Østergaard, M., S.J. Pedersen and U.M. Døhn, Imaging in rheumatoid arthritis – status and recent advances for magnetic resonance imaging, ultrasonography, computed tomography and conventional radiography. Best Practice & Research Clinical Rheumatology, 2008. 22(6): p. 1019-1044.
4. Porter-Young, F.M., et al., Inter- and intra-observer reliability of contrast-enhanced magnetic resonance imaging parameters in children with suspected juvenile idiopathic arthritis of the hip. Pediatric Radiology, 2018.
Figures