1376
Whole body MRI in myeloma: Optimising scan acquisition and read times.1Centre of Medical Imaging, University College London, London, United Kingdom
Synopsis
The study aim was to identify the highest value sequences for assessment of multiple myeloma by whole body MRI (WBMRI) to optimize scan acquisition and read times. Individual sequences (Dixon -/+ contrast, and diffusion imaging) were assessed in a prospective cohort of 29 patients with newly diagnosed multiple myeloma. Scan sensitivity, positive predictive value and reader confidence in detecting myeloma lesions and lesion conspicuity were assessed. Post-contrast water only Dixon and diffusion weighted images performed best. The results suggest that scan acquisition and read time can be reduced by focussing on WO contrast enhanced and diffusion images.
Introduction
Whole body MRI is recommended as the imaging modality of choice for the initial assessment of disease in patients with suspected myeloma (1,2). Detecting focal myeloma lesions is important as lesion number is a prognostic indicator (3). To facilitate the widespread use of WB-MRI, the ‘value’ must be optimised by using the most effective scan acquisition and read protocols. We have reviewed images acquired in an whole body protocol and compared lesion count, true positive rate, sensitivity, positive predictive value, conspicuity and read time for the different sequences to identify the highest yield images.Methods
Twenty-nine patients (12M:17F, median age 55, range 36-82) with biopsy-proven multiple myeloma underwent WBMRI imaging on a 3.0T wide-bore system (Ingenia; Phillips Healthcare, Netherlands). The WBMRI protocol included coronal pre- and post-contrast mDixon and diffusion weighted imaging covering the whole body.
The pelvic images from the whole-body datasets were reviewed. Unenhanced Dixon images [fat only (FO) and water only(WO)], post contrast Dixon (FOC and WOC) and DWI images from all 29 patients were randomised and read by three experienced readers. For each image type, the reader identified and labelled all visible myeloma lesions in the bony pelvis. Each identified lesion was compared with a reference standard consisting of pre- and post-contrast Dixon and diffusion weighted imaging which were read all together by a further specialist radiologist, to determine truly positive lesions. Lesion count, true positives, sensitivity, and positive predictive value (PPV) were compared across the image types. The time to read each scan set was recorded. Confidence for a diagnosis of myeloma was scored using a Likert scale. Lesion conspicuity was assessed by calculating percent contrast and contrast to noise ratio (CNR) of focal lesions in patients who did not have diffuse disease (n=13, total 151 myeloma lesions), using a previously described method (5). The Kruskal-Wallis test and Mann Whitney statistical tests was used to compare the various metrics across image types (statistical significance defined as p≤0.05).
Results
Three readers read 5 image types for 29 patients and identified 1098, 1265 and 1058 lesions, compared to 1852 reference lesions.
The mean lesion count, sensitivity, true positives, PPV and confidence scores for all three readers is summarised in Figure 2 and 3.
Significantly more lesions were identified on DWI compared to FO (p=0.014), WO (p=0.005) and FOC (p=0.01). Sensitivity and true positives were both significantly higher on DWI compared to all other image types (p values from p<0.001 to 0.048). The mean confidence score was significantly higher for DWI compared to FO (p=0.03), WO (p<0.001) and FOC (p=0.001).
Sensitivity, true positives and PPV were significantly higher for WOC images than WO at p=0.013, p=0.029 and p=0.027 respectively.
There was no significant difference between FOC and FO images for lesion count (p=0.84), sensitivity (p=1.0), true positives (p=0.75), PPV (p=0.28) or confidence (p=0.28).
Percent contrast was highest for WOC at 60.8% (FO 41.5%, WO 12.5%, 38.7%, FOC 38.7%, DWI 51.8%) and was significantly higher than the WO (p<0.001), FO (p=0.05) and FOC (p=0.01). There was no significant difference between FO and FOC images.
CNR was highest for DWI images at 65.7 (values for each image type were, FO 58.0, WO 34.7, FOC 32.7, WOC 29.9) and was significantly higher than WOC (p=0.03), FOC (p=0.049), WO (p=0.05).
The average read time for each image type was: FO 98s, WO 77s, FOC 99s, WOC 84s and DWI 67s.
Discussion
These results show that lesion detection rates are highest on DWI, followed by post contrast WO images. This is concordant with the conspicuity analysis which showed that myeloma lesions demonstrated highest percent contrast on WOC and highest CNR on DWI. Inclusion of pre-contrast images does not appear to add to lesion detection or confidence. Readers should therefore preferentially interrogate DWI and WOC images to detect myeloma lesions. Reading only the 2 highest yield sequences reduces read time compared to reading all 5 image types for this single imaging station from average 151 s compared to 428 s. This result suggests that pre-contrast imaging should be excluded from WB-MRI scan protocols for myeloma.Acknowledgements
No acknowledgement found.References
1. Dimopoulos MA, Hillengass J, Usmani S, Zamagni E, Lentzsch S, Davies FE, et al. Role of Magnetic Resonance Imaging in the Management of Patients With Multiple Myeloma: A Consensus Statement. J Clin Oncol [Internet]. 2015 Feb 20 [cited 2018 Sep 27];33(6):657–64.
2. Myeloma: diagnosis and management | Guidance and guidelines | NICE. [cited 2018 Sep 27]; Available from: https://www.nice.org.uk/guidance/ng35
3. Walker R, Barlogie B, Haessler J, Tricot G, Anaissie E, Shaughnessy JD, et al. Magnetic resonance imaging in multiple myeloma: diagnostic and clinical implications. J Clin Oncol [Internet]. 2007 Mar 20 [cited 2016 Jun 30];25(9):1121–8.
4. Bray TJP, Singh S, Latifoltojar A, Rajesparan K, Rahman F, Narayanan P, et al. Diagnostic utility of whole body Dixon MRI in multiple myeloma: A multi-reader study. Jiang Q, editor. PLoS One [Internet]. 2017 Jul 3 [cited 2018 Sep 27];12(7):e0180562.
5. Takasu M, Tamura T, Kaichi Y, Tanitame K, Akiyama Y, Date S, et al. Magnetic resonance evaluation of multiple myeloma at 3.0 Tesla: how do bone marrow plasma cell percentage and selection of protocols affect lesion conspicuity? PLoS One [Internet]. 2014 Jan [cited 2016 Apr 16];9(1):e85931.
Figures


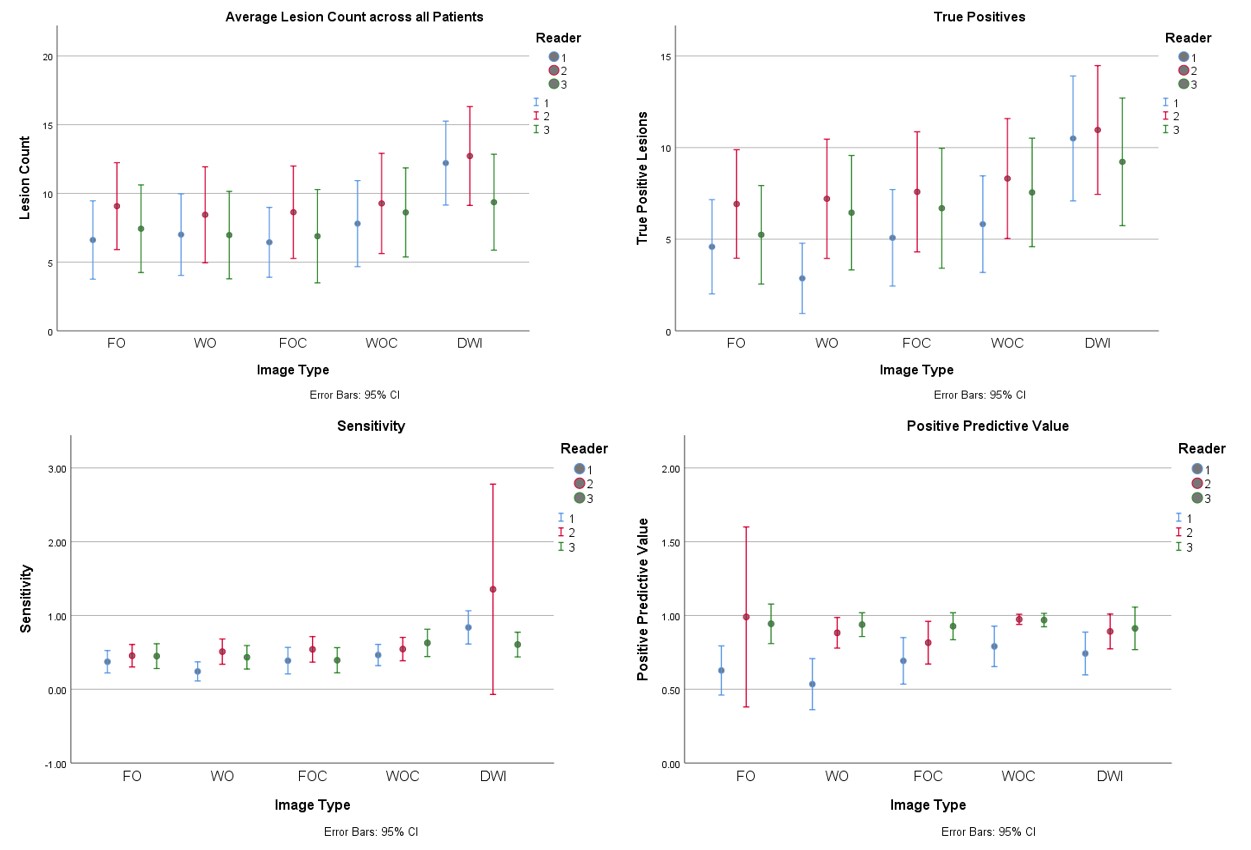
Average lesion count, sensitivity, true positive lesion count and positive predictive value (PPV) for each image type displayed for each of the three readers across all 29 patients.
Error bars indicate the 95% confidence interval.
Sensitivity and true positive lesion count were significantly higher for DWI compared to all image types (p values from p<0.001 to 0.048).
