1367
Assessment of the influence of metabolic syndrome on hip osteoarthritis by magnetic resonance imaging in subjects from the general population.1Department for Diagnostic and Interventional Radiology, University Hospital Tuebingen, Tuebingen, Germany, 2Department for Trauma and Reconstructive Surgery, BG Trauma Center Tuebingen, Tuebingen, Germany, 3University Hospital Munich, Munich, Germany, 4Department for Diagnostic and Interventional Radiology, Univeristy Hospital Tuebingen, Tuebingen, Germany, 5Radiology, University Hospital Freiburg, Freiburg, Germany
Synopsis
With being two of the leading chronic diseases, the purpose was to evaluate the effect of the metabolic syndrome on osteoarthritis of the hip in a healthy sample from the general population. Osteoarthritis was assessed according to the Kellgren-Lawrence classification, while the components of the metabolic syndrome were obtained as part of the clinical study protocol. Blood glucose was found to be a borderline non-dependent factor, while there was no correlation for waist circumference, triglyceride, blood pressure, and HDL. The overall metabolic syndrome was also not significantly correlated. In conclusion, metabolic syndrome and osteoarthritis of the hip are not associated.
Introduction
Osteoarthritis and metabolic syndrome are two of the leading chronic diseases in developed countries1-4. Metabolic syndrome, a constellation of hazard factors leading to diabetes mellitus as well as to cardiovascular disorders, contains common risk factors such as increased blood glucose levels, elevated waist circumference (central obesity), elevated blood pressure, increased triglycerides and lowered HDL5,6. Osteoarthritis is a major cause for a reduction in quality of life due to restriction in activity and disability7. Osteoarthritis and metabolic syndrome are often co-existent, whereby the direct impact on each other remains for the most parts unclear. There are multiple risk factors for developing osteoarthritis of the weight bearing joints (e.g. knee or hip joint), such as age, nutritional habits or central obesity which are concomitantly responsible for causing or worsening diabetes1,4.
Thus, the purpose was to investigate the effects of metabolic syndrome on osteoarthritis of the hip in a healthy cohort from the general population.
Method
Included were 354 asymptomatic subjects from KORA cohort (Cooperative Health Research in the Augsburg Region), which were classified as subjects with components of metabolic syndrome or healthy controls. Each subject underwent detailed assessment of waist circumference as well as fasting glucose to assess diabetic state, evaluation for systolic and diastolic hypertension, level of triglycerides and HDL as well as a full-body MR scan. MR measurements were performed on a 3 Tesla scanner (Magnetom Skyra, Siemens Healthcare, Erlangen, Germany) including a dual-echo Dixon and a T2 SS-FSE sequence for anatomical structures.
Evaluation of the images was performed by two radiologists with 3 and 11 years of experience in musculoskeletal imaging, independently. All cases were evaluated in a randomized and blinded fashion to the clinical data. To quantify osteoarthritis of the hip, assessment was performed with a modified Kellgren-Lawrence classification for osteophytes, joint gap narrowing and subchondral sclerosis.
In order to perform quality control as well as intrareader correlation, 40 participants were reevaluated in a blinded and randomized fashion by the primary reader.
Associations between metabolic syndrome components and hip degeneration were estimated by logistic regression models providing odds ratios.
Results
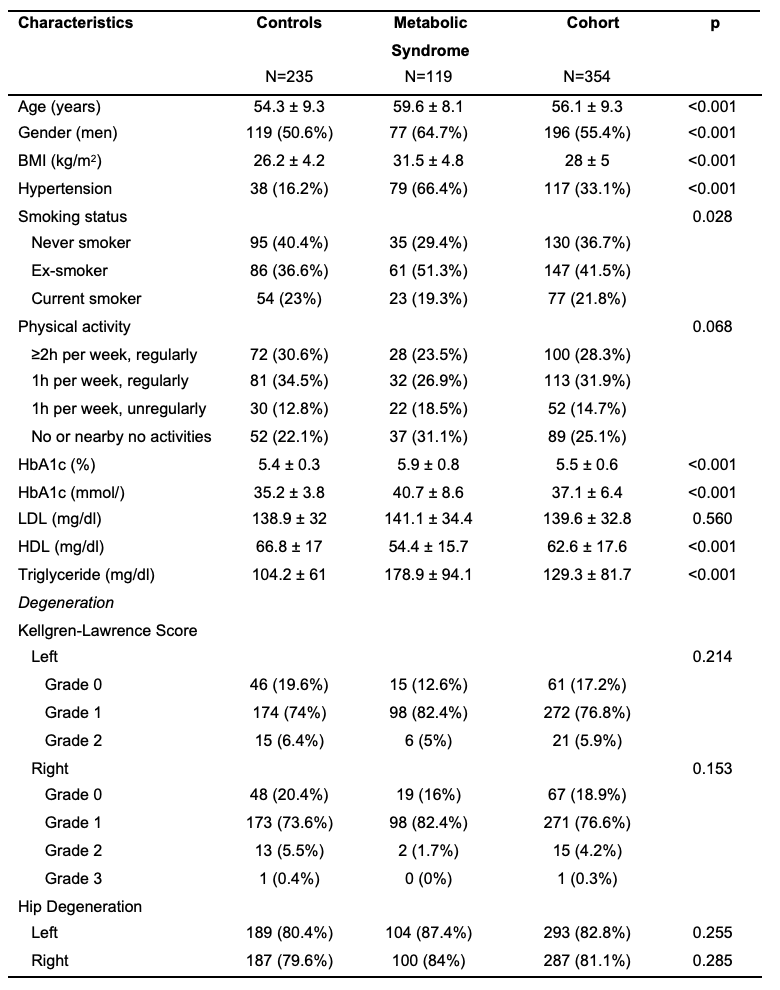
Of the included subjects, 119 (33.6%) were at risk for metabolic syndrome, while 235 (66.4%) were part of the healthy control group. Patient demographics and descriptive patient data about metabolic risk factors are given in Figure 1.
In total, the prevalence for osteoarthritis was 88.7%, with a prevalence for the right and left hip joint of 81.1% and 82.8%, respectively. In regards to the metabolic syndrome, therewas no significant difference in osteoarthritis of the hip joints compared to the healthy controls (p≥0.153; Figure 1). Furthermore, there was no significant difference between the metabolic syndrome group and controls regarding each criteria of the Kellgren-Lawrence classification, with osteophytes being borderline none significant (p≥0.053).
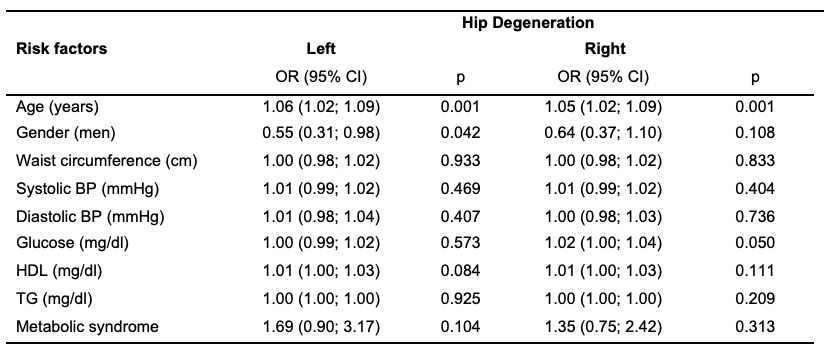
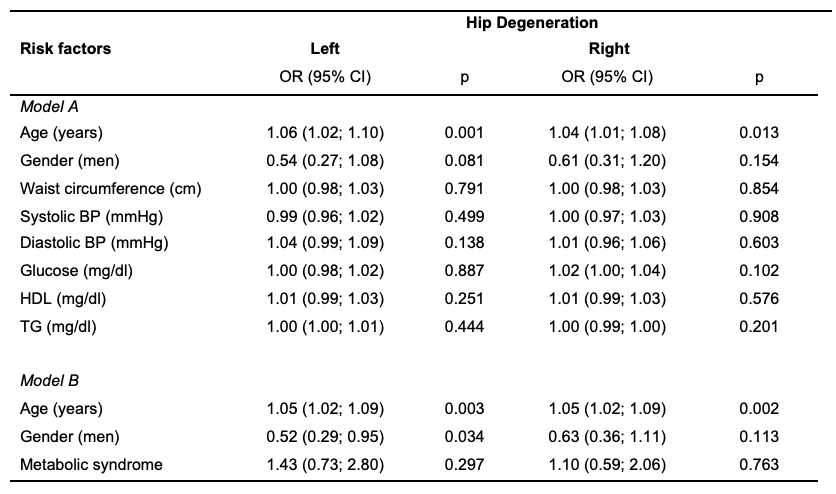
In univariate as well as multivariable analysis, age was significantly associated with osteoarthritis (p≤0.013) (Figure 2, 3). Furthermore, men showed significantly lower degeneration of the left hip in univariate analysis (p=0.042). However, this was only confirmed in Model B of the multivariable analysis (Figure 2, 3). Univariate correlations of the components of the metabolic syndrome and osteoarthritis of the hip joint showed only borderline non-significantly increased glucose levels for the right hip (p=0.05). None of the other components nor the overall metabolic syndrome showed a significant increase for osteoarthritis of the hip (Figure 2). Multivariable associations showed no significant difference, neither for one of the components nor overall metabolic syndrome (Figure 3).
Interreader agreement for osteoarthritis of the right (K=0.94) and left hip (K=0.88) was almost perfect. The same was seen for the degree of the Kellgren-Lawrence classification, with an almost perfect agreement for the right (K=0.86) and left hip (K=0.9). Furthermore, intrareader agreement was also almost perfect for the right (K=0.97) and left hip (K=0.96). The intrareader agreement for the degree of the Kellgren-Lawrence classification showed almost perfect agreement for the right (K=0.97) and left (K=0.96) hip joint, respectively.
Conclusion
Although influencing a wide range of diseases, metabolic syndrome and osteoarthritis of the hip joint are not associated.
Acknowledgements
No acknowledgement found.References
1. Schett G, Kleyer A, Perricone C, Sahinbegovic E, Iagnocco A, Zwerina J, et al. Diabetes is an independent predictor for severe osteoarthritis: results from a longitudinal cohort study. Diabetes Care. 2013;36(2):403-9.
2. Piva SR, Susko AM, Khoja SS, Josbeno DA, Fitzgerald GK, Toledo FG. Links between osteoarthritis and diabetes: implications for management from a physical activity perspective. Clin Geriatr Med. 2015;31(1):67-87, viii.
3. Louati K, Vidal C, Berenbaum F, Sellam J. Association between diabetes mellitus and osteoarthritis: systematic literature review and meta-analysis. RMD Open. 2015;1(1):e000077.
4. King KB, Rosenthal AK. The adverse effects of diabetes on osteoarthritis: update on clinical evidence and molecular mechanisms. Osteoarthritis Cartilage. 2015;23(6):841-50.
5. Olokoba AB, Obateru OA, Olokoba LB. Type 2 diabetes mellitus: a review of current trends. Oman Med J. 2012;27(4):269-73.
6. Alberti KG, Eckel RH, Grundy SM, Zimmet PZ, Cleeman JI, Donato KA, et al. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation. 2009;120(16):1640-5.
7. Zhang YM, Wang J, Liu XG. Association between hypertension and risk of knee osteoarthritis: A meta-analysis of observational studies. Medicine (Baltimore). 2017;96(32):e7584.
Figures