1352
A 1x1x1mm isotropic resolution CUBE-FLEX for imaging piriformis syndrome1Radiology, Stanford University, Stanford, CA, United States
Synopsis
Piriformis syndrome is one of the more common causes for sciatica-type symptoms, defined as impingement of the sciatic nerve by the piriformis muscle. MRI can be very useful in identifying the causative anatomic configuration for presurgical planning, but the conventional 2D sequences can be very challenging for the evaluation of the complex oblique anatomy of the piriformis muscle and sciatic nerve. We present a 5-minute isotropic resolution (1mm3) 3D fast-spin-echo sequence with fat-water separation, allowing arbitrary reformats to specify the causative anatomy as well as T2-weighted contrast to detect abnormal signal of the nerve in the context of associated neuropathy.
Introduction
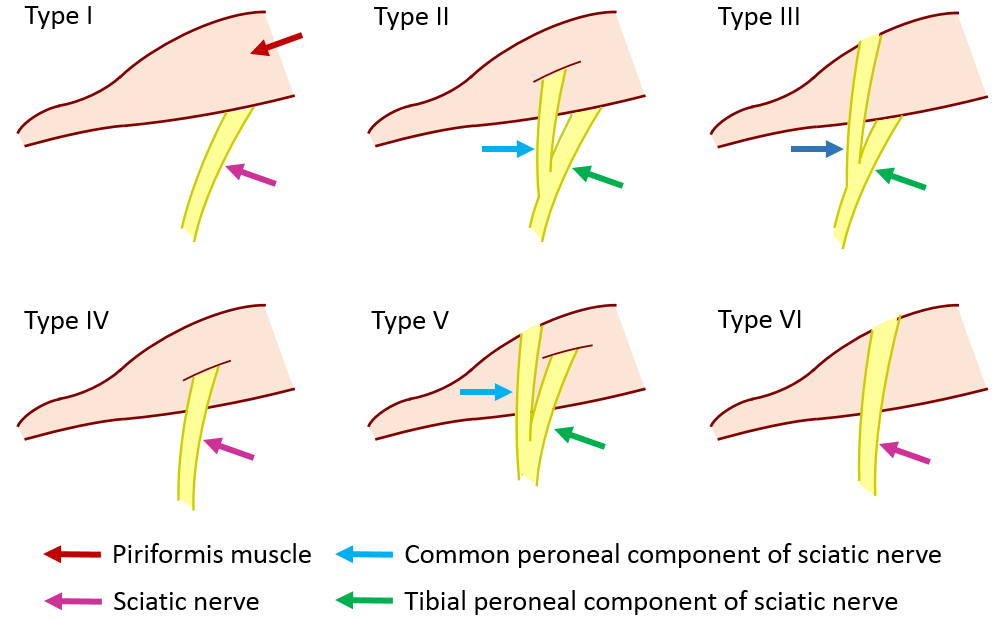
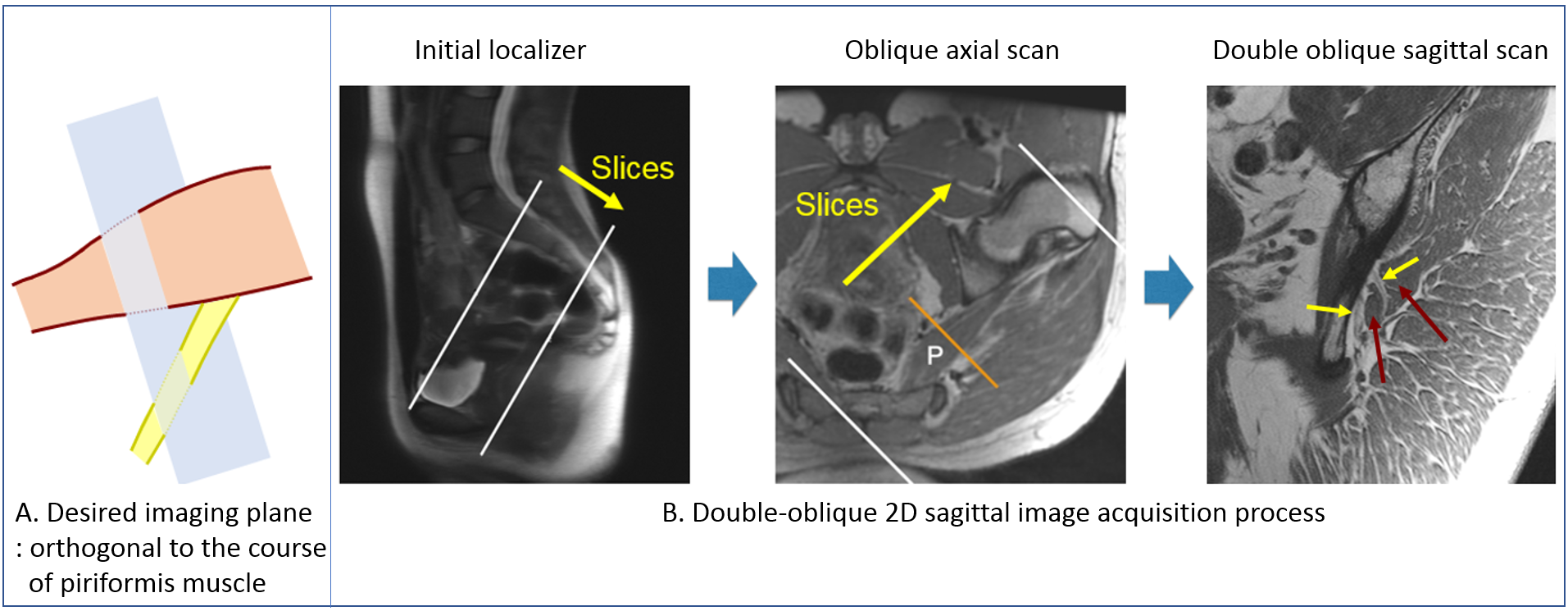
Piriformis syndrome is one of the major causes of sciatica, a common chronic pain condition on the sciatic nerve with a lifetime incidence of 13% to 40%. The cause of piriformis syndrome is impingement of the sciatic nerve by the piriformis muscle, where multiple forms of impingement exist due to various anatomic configurations (Fig.1)1-2. The excellent contrast of MRI between fat, muscle, and nerve makes MRI very useful for specifying the causative anatomic variant for surgical planning. The ideal imaging plane for this purpose would be the one orthogonal to the course of the piriformis muscle (Fig. 2). Unfortunately, the double-oblique course of the piriformis muscle requires two scout scans to prescribe the final double-oblique 2D sagittal scan, making the total exam very lengthy and error-prone. In this study, we introduce a novel configuration of a 3D fast-spin-echo sequence (CUBE) with Dixon-based fat-water separation (FLEX) with isotropic high resolution (1mm3) for imaging piriformis syndrome. Our approach demonstrated the feasibility for 1) specifying the anatomic variant type by reformatting on an arbitrary plane and 2) examining of potential neuritis with T2w-contrast in a 5-minute single scan.Methods
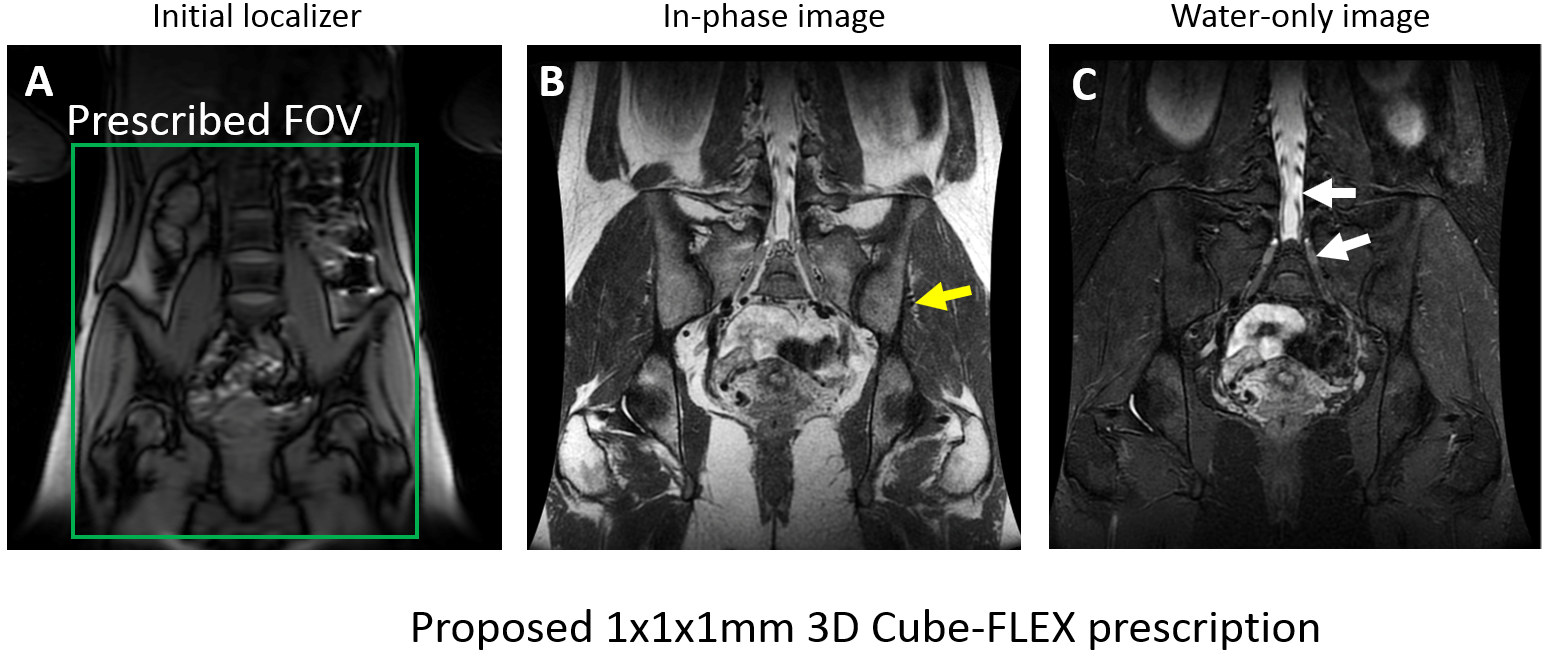
A 3D coronal isotropic fast-spin-echo sequence with Dixon-based fat-water separation was configured using a product sequence (CUBE) from a GE HD750 3T scanner. We adopted a bipolar readout to acquire both in-phase and out-of-phase signal in each echo of the echo train to restrict the scan time to 5 minutes and mitigate the motion-induced misregistration. A high bandwidth (200KHz) was selected to minimize the fat-blur and maximize the resolution along the frequency-encode direction. Out-of-volume suppression was employed to phase-encode only from the left greater trochanter to the right greater trochanter (Fig 3A). The rest of scan parameters were: TR/TE 2.5s/64ms, ETL 92, FOV 32x28.8x14.4cm, acquisition matrix 320x288x144, resolution 1x1x1mm, undersampling factor 2x2. A 32-channel body coil was used for imaging.Two healthy volunteers were recruited to test our sequence after signing an informed consent form reviewed by the Stanford institutional review board. Horos image analysis software (www.horosproject.org) was used for the double-oblique reformat of the acquired images to estimate the variant type. The estimated variant type was compared to that from a reference acquired from a double oblique sagittal T1-weighted 2D fast-spin-echo scan (Fig.2B).Results
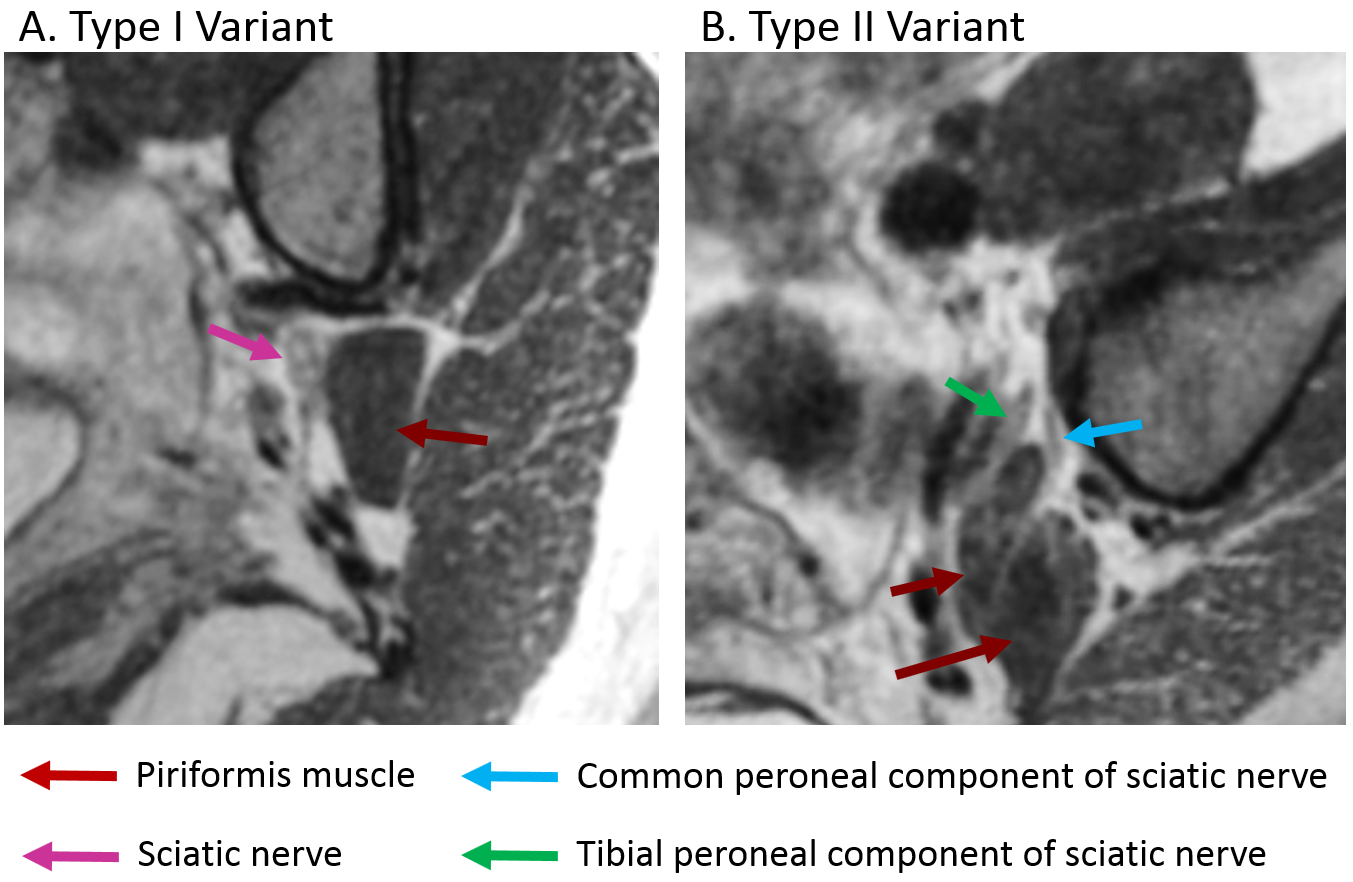
Fig.3B shows clear contrast between the fascial fat and the surrounding muscles (yellow arrow) in the in-phase image. Fig. 3C presents the fluid-sensitivity in the water-only image by high signal magnitude on CSF and dorsal root ganglions (white arrows). The fat contrast in the in-phase image was used to identify the split of the piriformis muscle and the sciatic nerve components for the variant type estimation. Fig.4 demonstrates the estimated variant type of each subject from the reformatted CUBE images, which coincided with the reference from the oblique T1 scans. Fig 4A shows the type I variant where the whole sciatic nerve exits on the inferior side of the piriformis muscle. Fig 4B shows the type II variant where the tibial component of the sciatic nerve runs on the inferior side of the piriformis muscle while the common peroneal component penetrates the piriformis muscle.Discussion
In this study, we introduced a novel configuration of the 3D fast-spin-echo sequence for piriformis syndrome. In a typical clinical scenario, it is unlikely that imaging is ordered after the diagnosis of piriformis syndrome is confirmed. Therefore, MR exams aim to offer the investigation of both the anatomic variant to help surgical planning in case piriformis syndrome is confirmed later and the abnormal nerve signal by other possible neuropathies. Our solution approach is to implement these two aims in a short single T2-weighted 3D sequence with Dixon-based fat-water separation by utilizing 1) the high fascial fat contrast of the in-phase image to identify the specific splitting pattern of the piriformis muscle and sciatic nerve and 2) the T2 contrast of the water-only image to detect abnormal nerve signal due to potential neuropathies. Our configuration of isotropic high resolution acquisition (1mm3) allowed reformatting images on the desired oblique imaging plane to facilitate the anatomic investigation. The adoption of fast bipolar readout was important in limiting the scan time to 5 minutes for practicality. In case of bilateral sciatic nerve examination, our sequence may replace one scouting scans (2 mins) and two oblique scans (5x2 = 10mins), which, in total, takes about 12 minutes.Conclusion
In summary, we have demonstrated the feasibility of an isotropic 3D fast-spin-echo sequence with Dixon-based fat-water separation to facilitate the examination of piriformis syndrome with a single 5 minute scan.Acknowledgements
NIH R01 AR0063643, NIH P41 EB015891, GE Healthcare.References
1.Beaton LE, Anson BJ (1937) The relation of the sciatic nerve and of its subdivisions to the piriformis muscle. Ant Rec 70:1-5.
2.Beaton LET, Anson BJ (1938) The sciatic nerve and the piriformis muscle: their interrelation a possible cause of coccygodynia. JBBS 20:686-688
Figures