1351
MRI Differentiation of Morel-Lavallee Lesions from Prepatellar Bursitis1Radiology, Mayo Clinic, Rochester, MN, United States
Synopsis
Differentiation of prepatellar bursitis from post-traumatic degloving injuries (Morel-Lavallee lesions) about the knee can occasionally present a diagnostic dilemma for clinicians and radiologists, although several features have been described as suggestive of a MLL etiology.
Our study adds to the evidence suggesting that intralesional fat globules and fluid extension beyond the confines of the normal prepatellar bursa are common findings in MLL lesions about the knee and suggestive that a lesion is unlikely to be an isolated prepatellar bursitis.
INTRODUCTION
Differentiation of prepatellar bursitis from post-traumatic internal soft tissue degloving injuries, or Morel-Lavallée lesions (MLL), about the knee can present a diagnostic dilemma for clinicians and radiologists. The purpose of this study was to investigate the imaging features that may be useful in discriminating anterior knee MLL lesions from prepatellar bursitis. A secondary aim was to examine the imaging features of MLL lesions in other anatomic locations.METHODS
Our institutional imaging database and electronic medical record were retrospectively searched for patients with suspected MLL lesions at any body site and bursitis in the prepatellar bursa. MRI imaging features including location, presence of internal fat globules, presence of transverse extension to the level of the femoral epicondyles, size, and MRI signal characteristics were noted along with clinical history and any surgical/pathologic results if available. Subsequent clinical or surgical confirmation (including surgical debridement, repeated aspiration, or need for sclerotherapy) was recorded.RESULTS
Our search identified 91 patients [47 male, 44 female, mean age 43.4 ± 21.5 years (range, 11-81)] with an MRI documenting a measurable fluid collection suspected of being MLL; 44 were located in the prepatellar region and 47 were located elsewhere (most commonly the hip/pelvis). Nine prepatellar cases were confirmed, while there were 12 confirmed MLL lesions at other sites in the body (femoral peritrochanteric- 8, lower thigh-3, elbow-1). Twenty-eight patients [22 male, 6 female, mean age 53.8 yr ± 13.2 years (range, 17-74)] were identified with a measurable prepatellar fluid collection suspected of being a prepatellar bursitis, 6 of which were confirmed by clinical follow-up.
There was a statistically significant difference in the presence of fat globules between confirmed prepatellar MLL (6/9, 67%) and prepatellar bursitis cases (0/6, 0%), p = 0.03. Internal fat globules were also found in the majority of confirmed MLL cases at other sites (9/12, 75%). Of suspected, but unconfirmed prepatellar bursitis cases, only 3/22 (13%) demonstrated internal fat globules, while 20/35 (57%) suspected but unconfirmed MLL cases showed internal fat (p = 0.002).
Transverse extension of prepatellar fluid to the level of the femoral epicondyles was more common in confirmed MLL cases (9/9,100%) than prepatellar bursitis cases (0/6 , 0%), p = 0.0002. Of suspected, but unconfirmed prepatellar bursitis cases, only 2/22 (9%) demonstrated transverse epicondylar extension, while 28/35 (80%) of suspected but unconfirmed MLL cases showed transverse epicondylar extension (p < 0.0001). 25/26 (96%) prepatellar MLL lesions with internal fat globules also demonstrated transverse extension to the femoral epicondyles. Confirmed MLL lesions demonstrated larger volume than prepatellar bursitis cases (61.6 +/- 59.8 cm3 vs. 13.1 +/- 8.2 cm3), which trended towards significance (p = 0.07).
There was no statistically significant difference in T1 signal intensity, T2 signal intensity, presence of fluid-fluid levels, enhancement pattern, or presence of surrounding edema between confirmed MLL and prepatellar bursitis patients.
DISCUSSION
This study confirms that there is significant overlap of MRI imaging features between prepatellar Morel-Lavallée lesions and prepatellar bursitis1,2. Transverse extension of a prepatellar fluid collection to the level of the femoral epicondyles (past the expected confines of the prepatellar bursa) was the most reliable discriminator between MLL and prepatellar bursitis, supporting results of a previous study3.
The presence of internal fat globules within the fluid collection was also significantly more common in MLL than bursitis, though was not 100% specific. Interestingly, we found that the vast majority of lesions (25/26, 96%) with internal fat globules also demonstrated transverse extension to the femoral epicondyles- we suspect that many of these represented MLLs, but were limited by a lack of clinical or surgical follow-up to enable confirmation. Examining the diagnostic accuracy afforded by a combination of these two imaging features in a larger cohort of confirmed cases would be beneficial.
Although conservative treatment including rest and compression are common for both MLL and prepatellar bursitis, improved diagnostic confidence can help facilitate appropriate follow-up and adjust the threshold and timing for intervention if early conservative treatment is unsuccessful.
CONCLUSION
Fluid collection extension beyond the normal confines of the prepatellar bursa to the level of the femoral epicondyles and the presence of internal fat globules are commonly seen in prepatellar Morel-Lavallée lesions, and are useful in discriminating these lesions from prepatellar bursitis.Acknowledgements
No acknowledgement found.References
1. Vassalou EE, Zibis AH, Raoulis VA, et al. Morel-Lavallée Lesions of the Knee: MRI Findings Compared With Cadaveric Study Findings. AJR Am J Roentgenol. 2018 May;210(5):W234-W239.
2. Rodrigo O. Aguiar, Flavio C. Viegas1, Rodrigo Y. Fernandez1, et al. The Prepatellar Bursa: Cadaveric Investigation of Regional Anatomy with MRI After Sonographically Guided Bursography. American Journal of Roentgenology. 2007;188: W355-W358.
3. Borrero CG, Maxwell N, Kavanagh E. MRI findings of prepatellar Morel-Lavallée effusions. Skeletal Radiol. 2008 May;37(5):451-5.
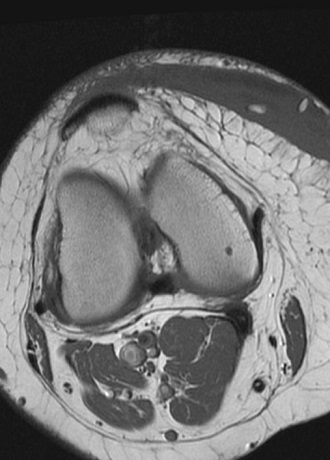
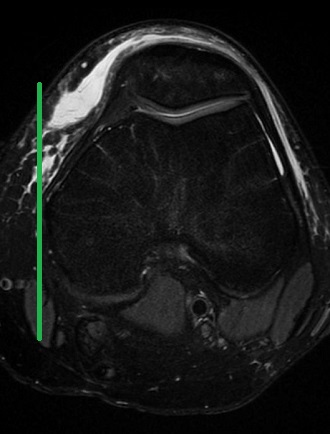
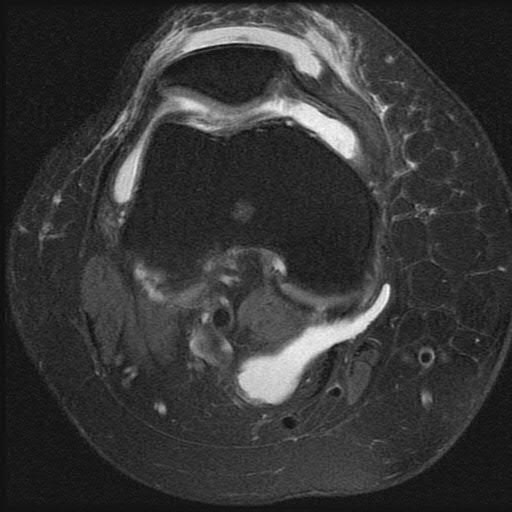
Figures