1348
How to segment muscle images using qNMRI to obtain the highest discriminant power in natural history studies of muscle diseases in adult patients?1NMR Laboratory, Neuromuscular Investigation Center, Institute of Myology, Paris, France, 2NMR Laboratory, CEA, DRF, IBFJ, MIRCen, Paris, France
Synopsis
Fat fraction (FF), as calculated from water-fat (Dixon) NMR images, is a largely accepted, if not fully validated, muscle imaging biomarker, which has been proposed as an outcome measure in most neuromuscular disorders these last few years. The question remains, however, as to whether specific muscle or muscle groups should be taken into consideration for longitudinal evaluation in specific neuromuscular diseases. Here, we looked into a cohort of patients suffering from three different neuromuscular disorders: immune-mediated necrotizing myopathy, (sporadic) inclusion body myositis and GNE myopathy. The aim of this work was to compare whole-segment FF with individual muscle and muscle group FF values and identify the most efficient procedure to quantify disease progression, by comparing the standardized response means.
Introduction
Fat fraction (FF), as calculated from water-fat (Dixon) NMR images1, is a largely accepted, if not fully validated, muscle imaging biomarker, which has been proposed as an outcome measure in most neuromuscular disorders these last few years2. The question remains, however, as to whether specific muscle or muscle groups should be taken into consideration for longitudinal evaluation in specific neuromuscular diseases. Most often all muscles are segmented and evaluated over a number of slices. Here, we looked into a cohort of patients suffering from three different neuromuscular disorders: immune-mediated necrotizing myopathy (IMNM)3, (sporadic) inclusion body myositis (IBM)4 and GNE myopathy (GNEM)5. All three pathologies are characterized by severe muscular lesions and muscle fatty replacement, although to different extents. The aim of this work was to compare whole-segment FF with individual muscle and muscle group FF values and identify the most efficient procedure to quantify disease progression, by comparing standardized response means (SRM).Methods
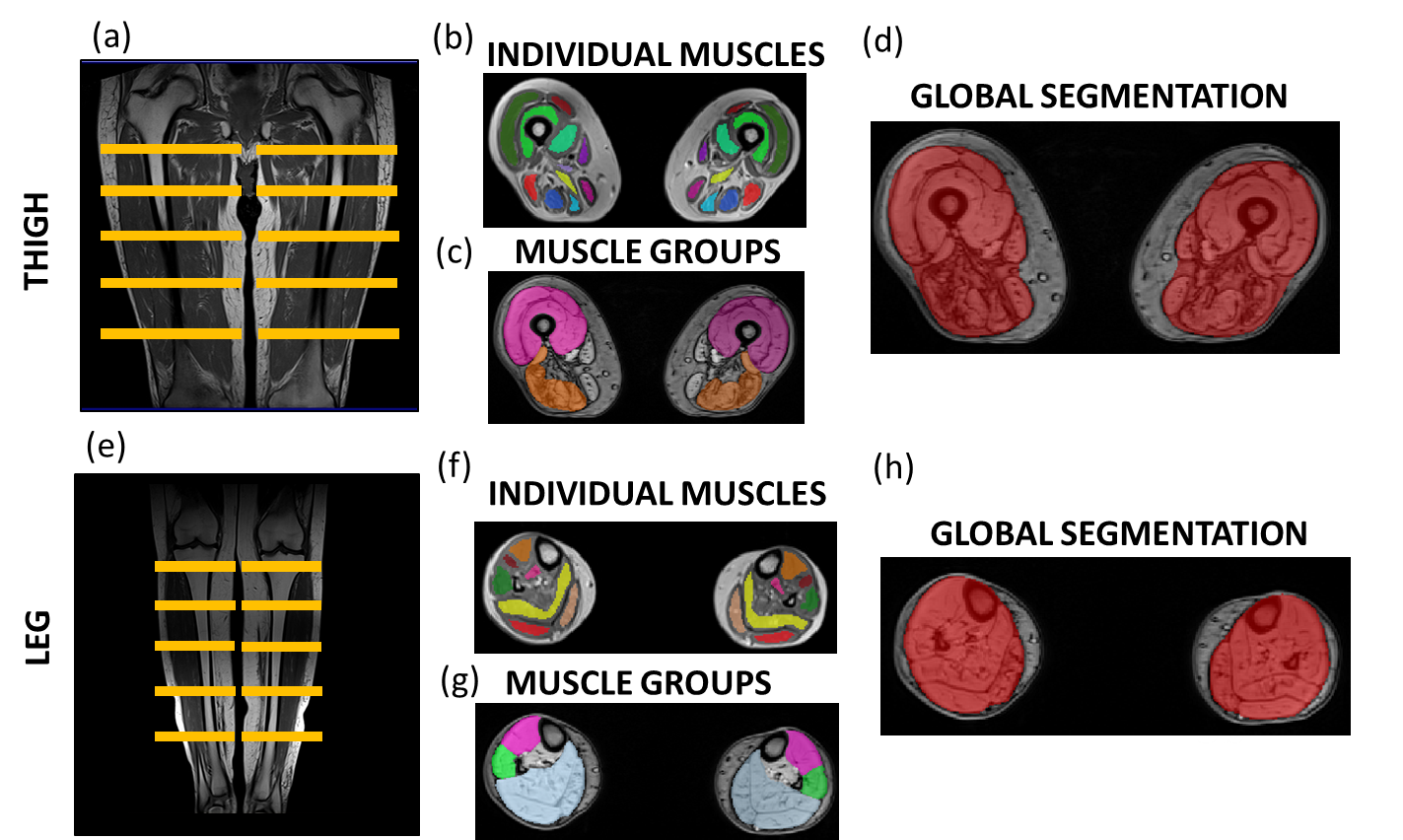
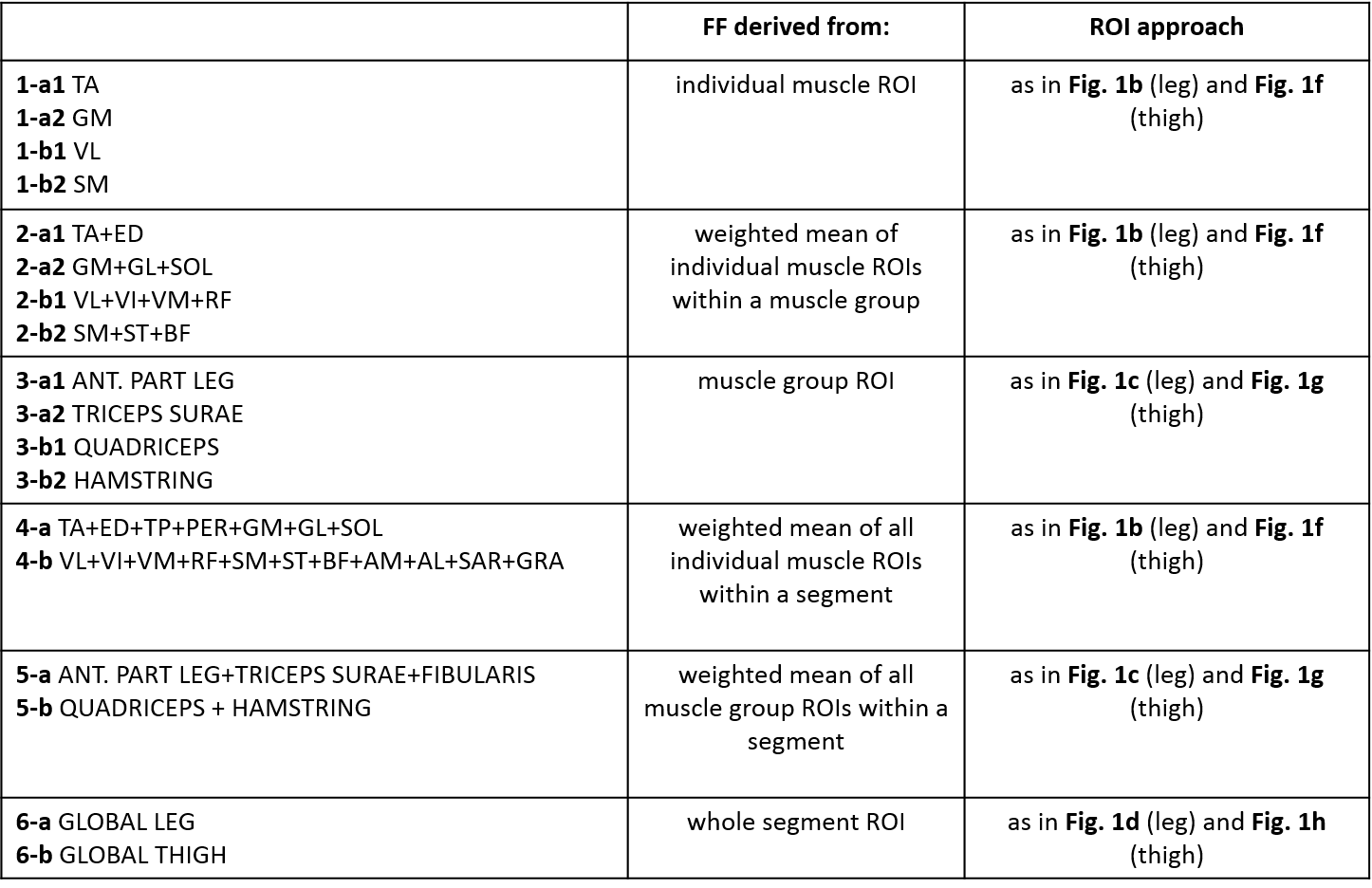
Sixteen IMNM patients (47±17 years old, age range: 18-74, 5 male), ten IBM patients (66±5 years old, age range: 18-75, 4 male) and 10 GNEM patients (47±14 years old, age range: 26-74, 5 male) were scanned twice within a one-year interval on a clinical 3T Siemens PrismaFit NMR system using a body matrix/spine coil. Patients were scanned as part of different natural history studies (without therapeutic intervention between baseline and year-1). A fat/water separation 3-point Dixon NMR sequence (at 3 different TEs = 2.75/3.95/5.15 ms, TR=10 ms) was performed in 5 slices at the level of the thigh and the leg (Fig. 1a/e). Regions of interest (ROIs) were drawn, using the out-of-phase Dixon images, in the different individual muscles (well inside the muscle avoiding subcutaneous (SC) fat), in muscle groups (including inter-muscular fat and fascia but avoiding subcutaneous fat), in weighted combinations of individual muscles and muscle groups, and the whole leg and thigh (including the femoral bone but avoiding subcutaneous fat), using an interactive manual segmentation tool itkSNAP (Fig. 1). From these ROIs, values for FF were derived. Changes in FF using all methods (individual, group, combinations of individuals and groups or whole as explained in Table 1) were compared using ANOVA (P<0.05). SRM is defined as the mean change in FF (ΔFF) divided by the mean standard deviation of ΔFF, and SRMs > 0.8 were evaluated as being highly responsive to ΔFF.Results
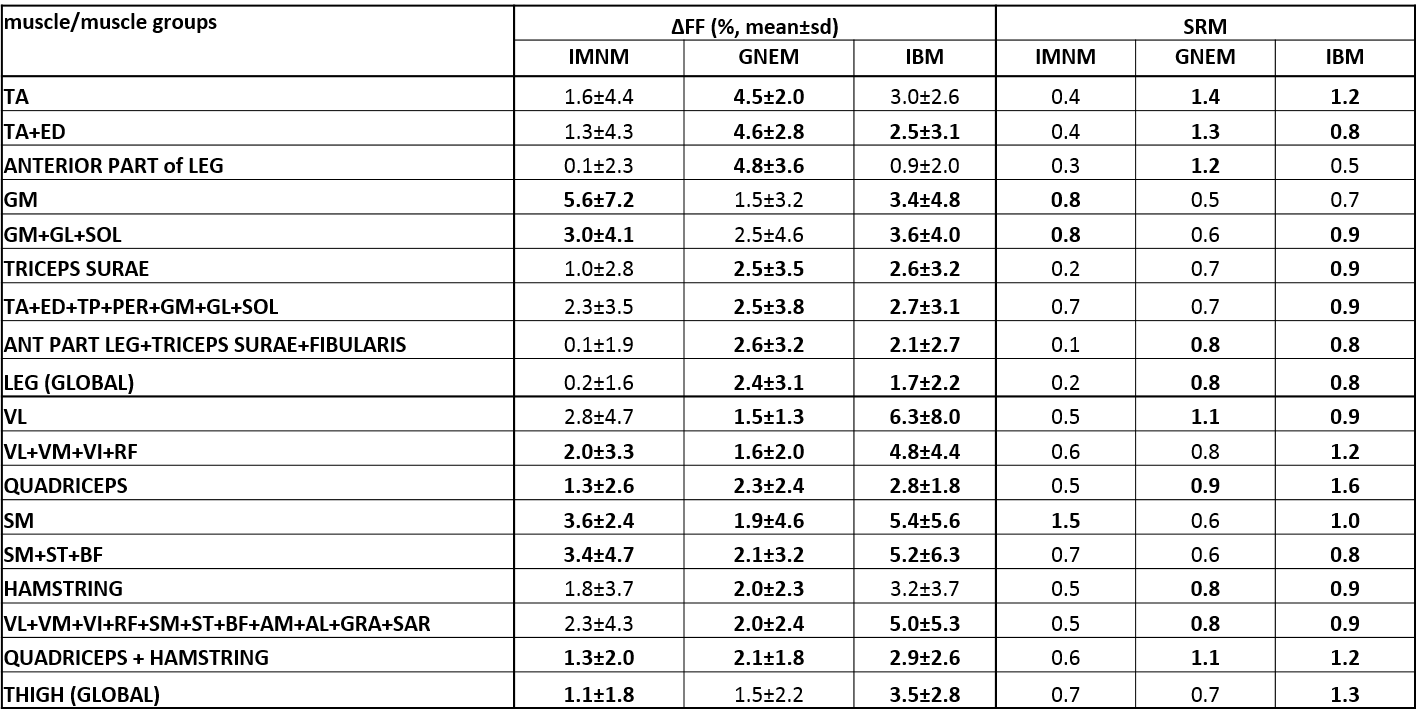
Table 2 gives an overview of the results. Whereas in IBM, SRM values were > 0.8 for almost all approaches, this was less the case for GNEM and IMNM. Global FF of the thigh is very sensitive in IBM patients although quadriceps FF gives slightly higher values. For GNEM patients, vastus lateralis or quadriceps is more sensitive to change in FF than global FF. In IMNM, semimembranosus FF seems a good candidate for evaluating the disease progression. In case of the leg is global FF sensitive enough to follow-up on disease progression in both IBM and GNEM, although tibialis anterior FF is also a good candidate. Similarly as for the thigh in IMNM, an individual muscle – in this case, gastrocnemius medialis, is the most sensible approach to evaluate the progression of the disease.Discussion & Conclusion
Using the SRMs to
evaluate the ability of various FF estimation procedures to monitor disease
progression, it appeared that the most sensitive approach depended on the
disease. Whereas global FF seems to be a good approach in IBM for both segments
but especially for the thigh, this is less the case for GNEM and IMNM. In the
case of GNEM leg, global FF is sensitive enough for tracking changes in FF,
although individual muscles such as tibialis anterior or the anterior leg muscle group give
higher SRM values. This suggests that individual muscle
segmentation – a tedious step in using qNMR imaging to characterize
muscle structural changes, is not always mandatory depending on the pathology.
There has also been a recurrent quest by investigators for the most appropriate
muscle (group) on which to focus the analysis. Other yet unpublished data in limb-girdle
muscular dystrophy types 2B and 2I patients showed that global approaches as we
found in IBM were associated with superior performance. Still, as based on our results, generalization
of the concept is premature in the present stage. Other conditions need to be
revisited. Because the global approach takes into
account intermuscular fat, changes in patient nutritional status will
likely bias the evaluation of muscular FF and the impact has to be carefully
determined. Applicability to contractile tissue indices and water T2
distribution has yet to be investigated. Also data in other neuromuscular diseases such as Duchenne/Becker
muscular dystrophy need to be investigated.Acknowledgements
No acknowledgement found.References
1. Dixon WT. Simple proton spectroscopic imaging. Radiology.1984,153(1):189-194.
2. Carlier PG, Marty B, Scheidegger O, et al. Skeletal muscle quantitative nuclear magnetic resonance imaging and spectroscopy as an outcome measure for clinical trials. J. Neuromuscul. Dis. 2016,3(1):1-28.
3. Pinal-Hernandez I, Casal-Dominguez M, Mammen AL. Immune-Mediated Necrotizing Myopathy. Curr. Rheumatol. Rep. 2018,20(4):21.
4. Naddaf E, Barohn RJ, Dimachkie MM. Inclusion Body Myositis: Update on Pathogenesis and Treatment.
Neurotherapeutics. 2018, Epub.
5. Eisenberg I, Avidan N, Potikha T, et al. UDP-N-acetylglucosamine 2-epimerase/N-acetylmannosamine kinase gene is mutated in recessive hereditary inclusion body myopathy. Nat Genet. 2001,29(1):83-87.
Figures