1346
Intramuscular magnesium measured by 31P-MRS is more closely associated with age and muscle function than is serum magnesium1National Institute on Aging, National Institutes of Health, Baltimore, MD, United States, 2Norwich Medical School, University of East Anglia, Norwich, United Kingdom, 3Radiology and Imaging Sciences, Emory University, Atlanta, GA, United States
Synopsis
We evaluate the relationships between muscle strength and intramuscular magnesium, measured by phosphorus magnetic resonance spectroscopy (31P-MRS), or serum magnesium. We further evaluate the relationships between these measures of magnesium status and age, sex, and muscle strength. Data were collected from participants in the Baltimore Longitudinal Study of Aging, a large cohort of normatively aging subjects encompassing a broad age range. Results showed that intramuscular magnesium was more closely associated with age and muscle function than was serum magnesium and may therefore represent a better clinical measure of magnesium status.
Introduction
Magnesium status is usually assessed by serum level; however, this pool represents only ~1% of total magnesium content and is not directly involved in muscle function. In contrast, the much larger intramuscular magnesium pool reflects intramuscular availability for actin/myosin crossbridge cycling and may therefore prove a much more appropriate measure of functional magnesium status. In this study, we used 31P-MRS to examine skeletal muscle magnesium status1, 2 and defined its relationship with serum magnesium, age, and muscle function in a group of healthy men and women over a wide age range.Methods
Data were obtained from 459 participants (215 male, median [range] age = 73 [24–98] yrs) of the Baltimore Longitudinal Study on Aging (BLSA). Magnetic resonance spectroscopy (MRS) was performed using a Philips Achieva 3.0T X-series MRI scanner (Philips Healthcare, Best, NL) with a 10-cm transmit-receive loop coil (PulseTeq, Surrey, UK). Pulse-acquire 31P spectra were obtained from the left thigh with the following sequence parameters: repetition time = 25s, spectral bandwidth = 2250Hz, 2048 sampled points, 4 signal averages, and an adiabatic excitation pulse with a flip angle of 90°. A long repetition time was chosen to obviate the need for relaxation correction of metabolite ratios. Additionally, we measured serum [Mg2+] using a conventional clinical colorimetric assay, and maximum quadriceps muscle strength using an isokinetic dynamometer, with left-leg knee extensor contractions performed at a knee flexion of 70°.
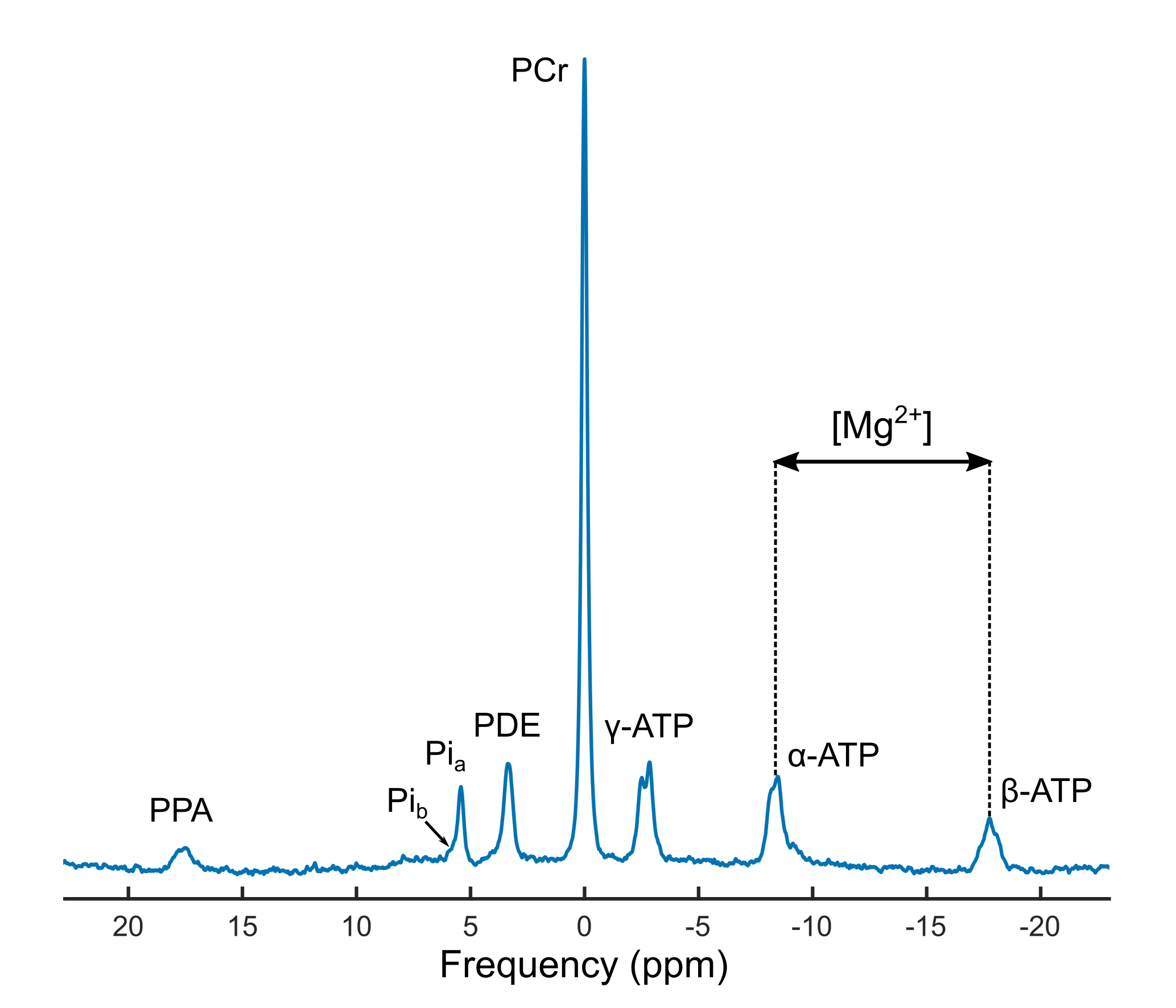
Spectra were processed using in-house software written in Python. Processing included 8Hz Lorentzian apodization, two-times zero-filling, and zero- and first-order phase correction, and spectral line amplitudes and chemical shifts were calculated using the AMARES algorithm within jMRUI (version 3.0, www.jmrui.eu). The chemical shifts of the two inorganic phosphate resonances were then used to calculate a weighted pH, as previously described.3 The free intracellular magnesium concentration was estimated using the quadratic equation given by Wary et al.1, incorporating the observed chemical shift of β-ATP relative to α-ATP, the weighted pH, and a set of known chemical shifts and formation constants from the literature.4
Statistical analyses were performed in R (version 3, R Foundation for Statistical Computing, Vienna, Austria). Cross-sectional relationships were evaluated using linear regression, with standardized variables used to permit comparison of effect size, defined as the slope, β, of the regression.
Results/Discussion
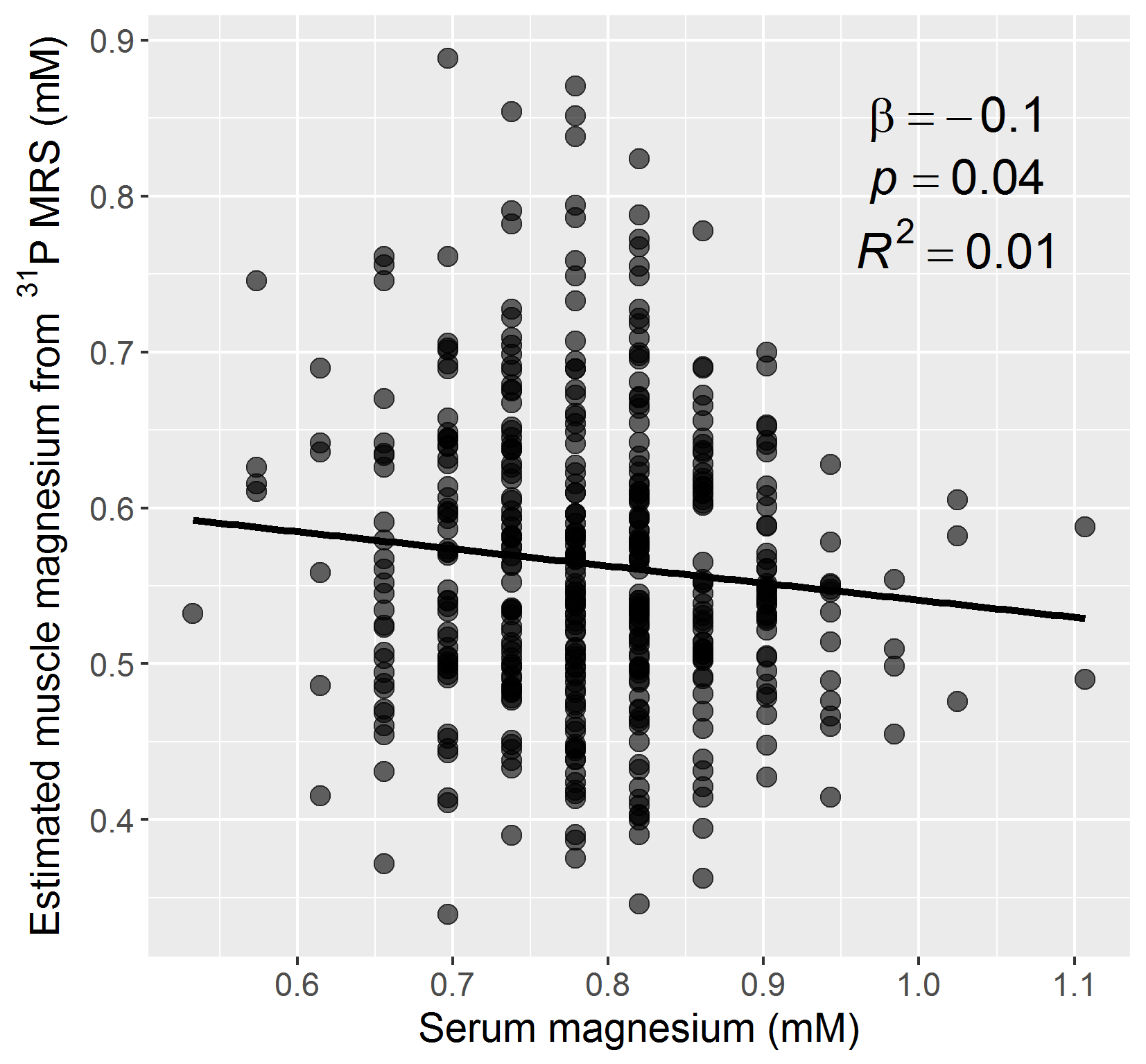
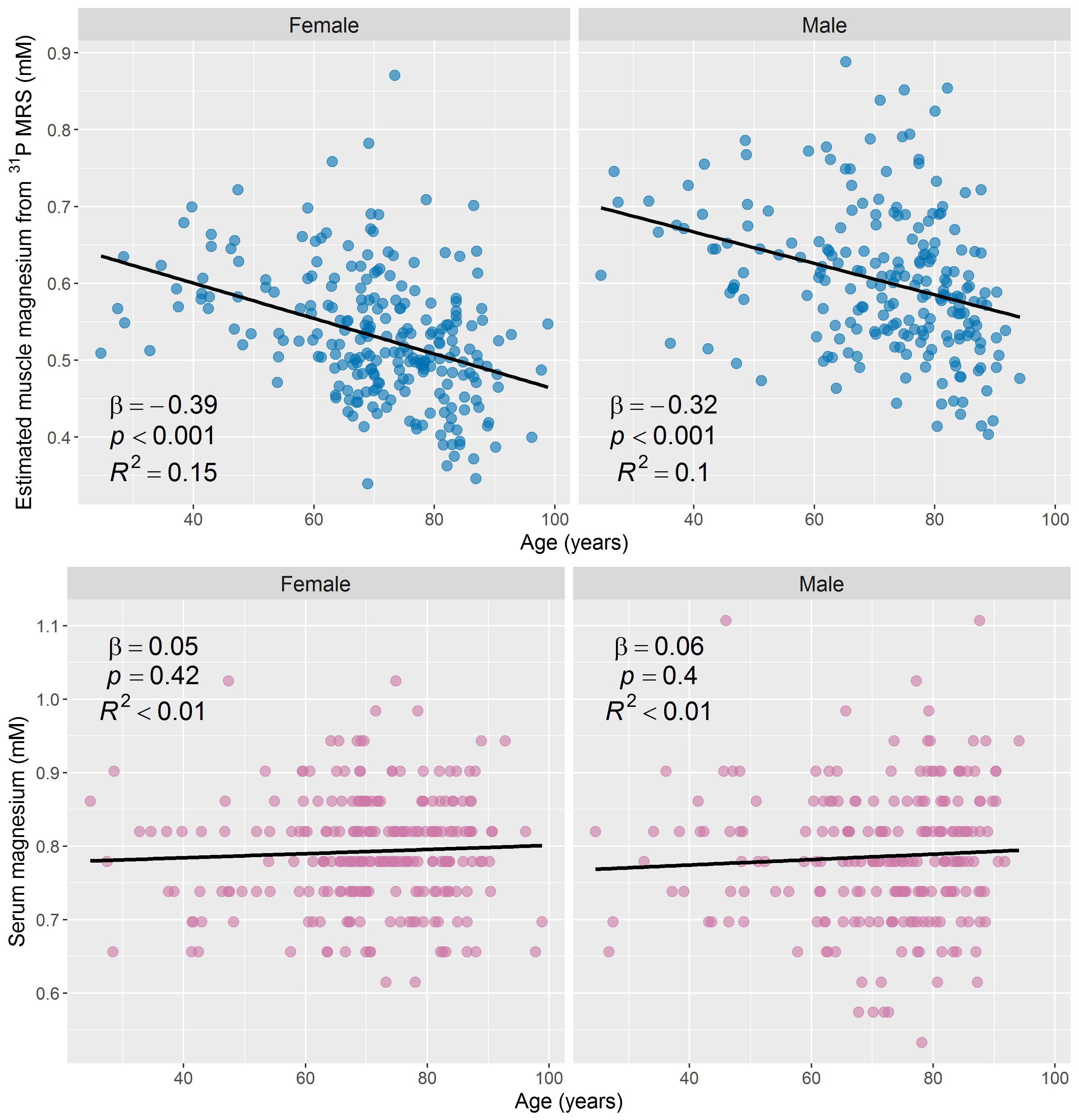
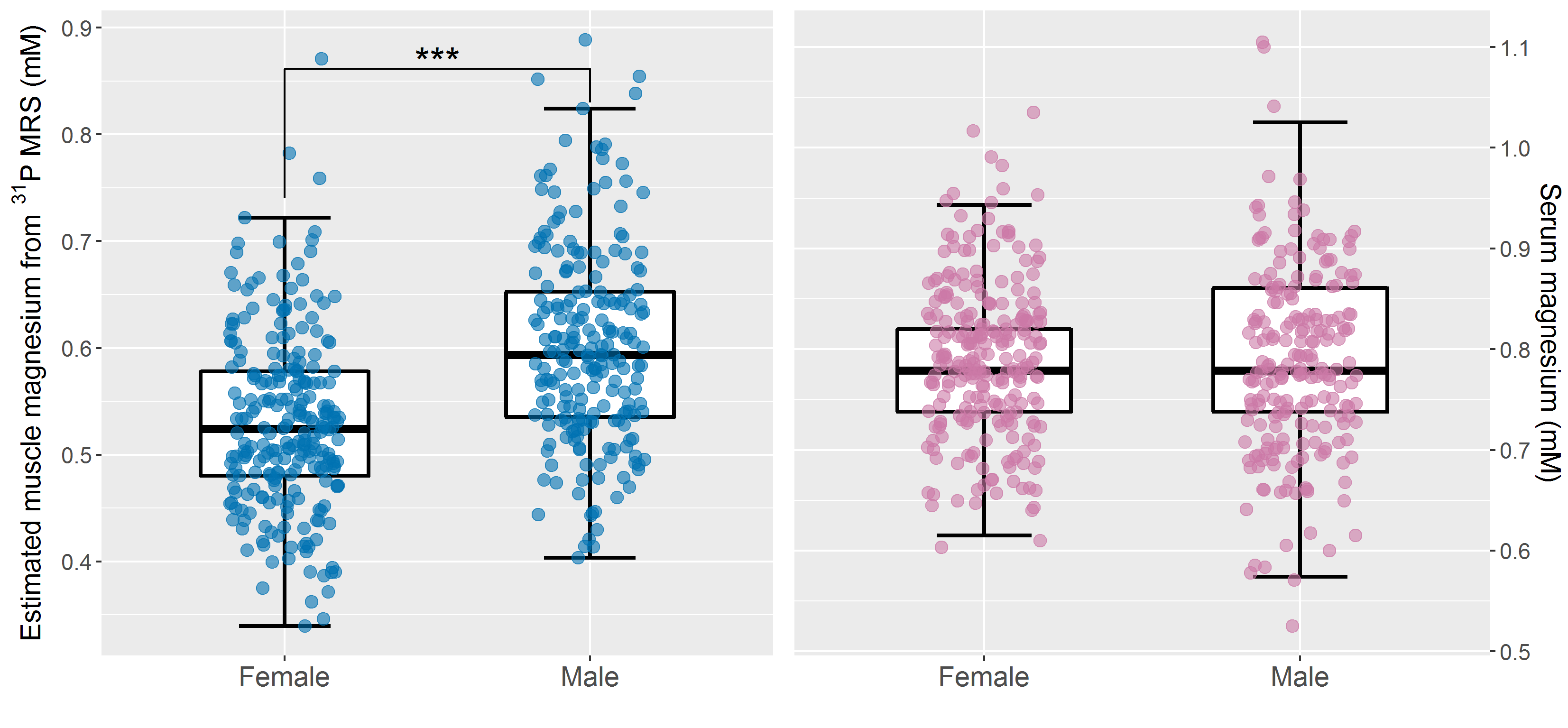
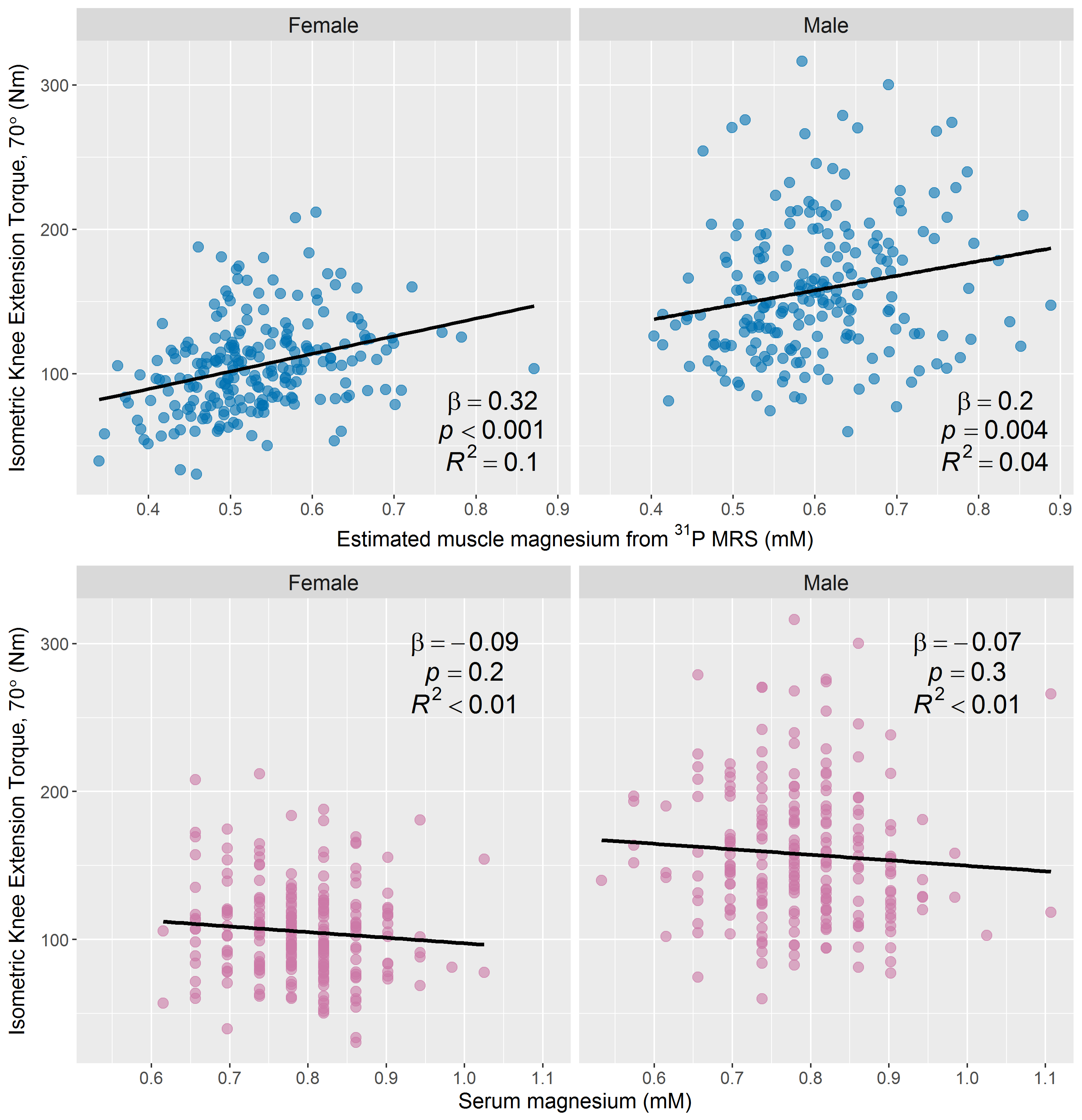
Figure 1 shows a representative 31P-MRS spectrum. Intramuscular [Mg2+] was inversely associated with serum [Mg2+], as shown in Figure 2. There was a statistically-significant negative association between intramuscular [Mg2+] and age, with β=−0.31, p<0.001, and R2=0.09; this association remained significant after stratifying by sex, as illustrated in Figure 3, and there was a significant difference in regression slopes between the two sexes (p<0.001). Furthermore, a Mann-Whitney U test indicated a statistically-significant difference in intramuscular [Mg2+] between male and female participants (Figure 4). Conversely, serum [Mg2+] was not significantly associated with age, and there were no sex differences. Finally, intramuscular [Mg2+] was associated with knee-extension torque in male and female subgroups (β=0.18, p=0.01, R2=0.06; and β=0.35, R2=0.12, p<0.001, respectively, adjusting for BMI), while serum [Mg2+] showed no association (Figure 5).
Previous work by Dominguez et al. showed an association between serum magnesium and muscle strength in the InCHIANTI study of aging.5 In the present work, serum magnesium was not significantly associated with knee extension strength; however, the BLSA represents an exceptionally healthy cohort. Our 31P-MRS measures of intramuscular magnesium were associated with muscle strength in this healthy group and may thus provide valuable clinical insight into the etiology of muscle dysfunction.
Conclusion
We found that intramuscular magnesium was more strongly associated with age and muscle function than was serum magnesium. As such, our 31P-MRS measures of muscle magnesium will be invaluable for assessing muscle changes with age, improving our understanding of sarcopenia and frailty, and permitting testing of dietary, exercise, and pharmaceutical interventions.Acknowledgements
This research was supported entirely by the Intramural Research Program of the NIH, National Institute on Aging. We acknowledge Pierre Carlier and Harmen Reyngoudt for their advice regarding magnesium determination with 31P-MRS.References
1. Wary C, Brillault-Salvat C, Bloch G, Leroy-Willig A, Roumenov D, Grognet J, et al. Effect of chronic magnesium supplementation on magnesium distribution in healthy volunteers evaluated by 31P-NMRS and ion selective electrodes. British Journal of Clinical Pharmacology. 1999;48(5):655.
2. Iotti S, Frassineti C, Alderighi L, Sabatini A, Vacca A, Barbiroli BJMri. In vivo 31P-MRS assessment of cytosolic [Mg2+] in the human skeletal muscle in different metabolic conditions. Magnetic Resonance Imaging. 2000;18(5):607-14.
3. Reyngoudt H, Turk S, Carlier PG. 1H NMRS of carnosine combined with 31P NMRS to better characterize skeletal muscle pH dysregulation in Duchenne muscular dystrophy. NMR in Biomedicine. 2018;31(1):e3839.
4. Halvorson H, Vande Linde A, Helpern J, Welch K. Assessment of magnesium concentrations by 31P NMR in vivo. NMR in Biomedicine. 1992;5(2):53-8.
5. Dominguez LJ, Barbagallo M, Lauretani F, Bandinelli S, Bos A, Corsi AM, et al. Magnesium and muscle performance in older persons: The InCHIANTI study. The American Journal of Clinical Nutrition. 2006;84(2):419-26.
Figures