1343
Intravoxel Incoherent Motion (IVIM) Perfusion Imaging of the Shoulder Muscles Activated by Tennis Playing: Initial Results1Institute for Biomedical Engineering, University and ETH Zürich, Zürich, Switzerland, 2University of Zürich, Zürich, Switzerland, 3Radiology, University Hospital of Basel, Basel, Switzerland
Synopsis
Playing tennis involves complex simultaneous motion patterns of several muscles of the shoulder. Intravoxel incoherent motion (IVIM) perfusion imaging offers the possibility to map muscle activation by measuring changes in local blood flow. In this preliminary work four healthy right-handed volunteers were examined after tennis exercises using IVIM perfusion imaging. The results indicate a particular use of m. subscapularis and m. pectoralis major during forehand strokes and of the of m. subscapularis during service.
INTRODUCTION
The muscular involvement during movements of the shoulder such as playing tennis are complex because several muscles participate in stabilization and motion. Better understanding of the muscle usage during tennis exercises may help to prevent injuries, improve regeneration and training efficiency of athletes. Intravoxel incoherent motion (IVIM) perfusion imaging offers the possibility to measure the activation of deep lying muscles indirectly by changes of local blood flow.1,2 The aim of this work was to study the influence of different tennis strokes on the activation of muscles assessed by IVIM blood flow related fD* perfusion imaging.
METHOD AND MATERIALS
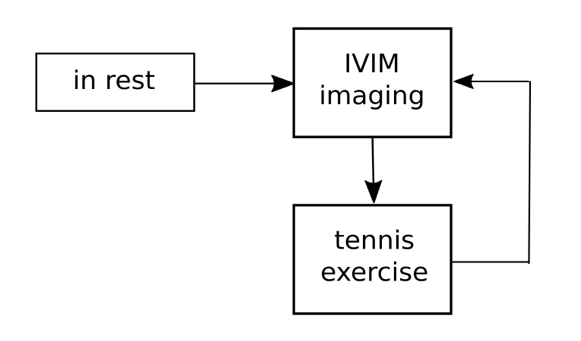
Imaging: Four male right-handed volunteers (22±2y) with prior experience in tennis were scanned at a 3T Achieva system (Philips Healthcare) using a 4-channel shoulder coil, first without performing exercises, and then immediately after playing forehand, backhand (double-handed) and service, respectively. Each tennis session took five minutes (approx. 60 strokes) with 20 minutes of pausing. A tennis-ball serving machine (miha 2002) was used to pass the ball to the volunteers in a repeatable way. Immediately after each session the right shoulder of the volunteer was scanned using an IVIM diffusion-weighted sequence consisted of a spin-echo with echo planar readout and monopolar pulsed gradients with 12 b-values (0, 10, 20, 40, 80, 110, 140, 170, 200, 300, 400 and 500 s/mm2) in six directions. In order to gather anatomical information a T1-weighted turbo spin-echo sequence was performed afterwards.
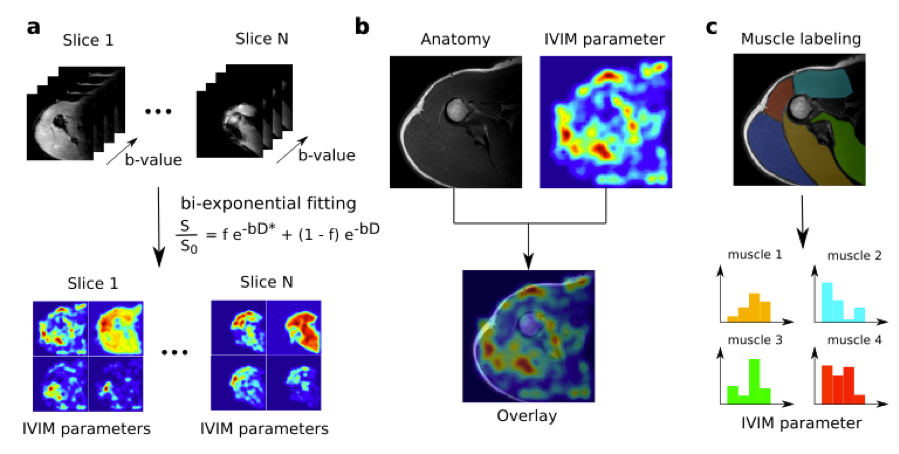
Post-processing: The IVIM bi-exponential signal equation model was fitted using a Matlab implementation of a standard two step algorithm. In the first step D was fitted using a mono-exponential signal equation on values b > 200 s/mm2, and in the second step, fD* was determined during which D as acquired in the first step was kept fixed. The bi-exponential model was fitted on the traces of all b-values.
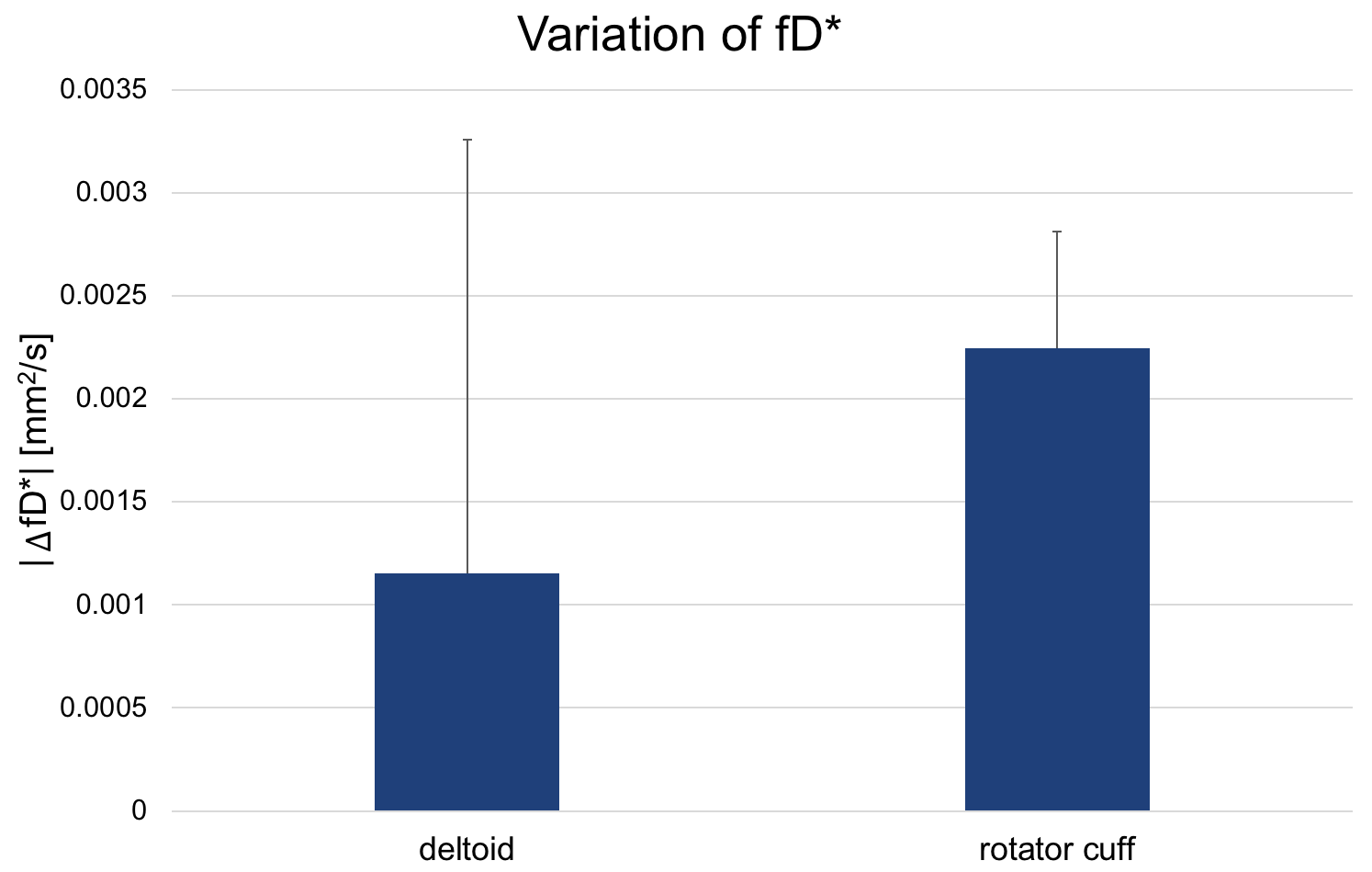
Quantitative analysis: Regions of interest were drawn in the shoulder in order to assign the IVIM parameters to the corresponding muscles (m. infraspinatus, m. supraspinatus, m. subscapularis, m. deltoideus (posterior, lateral and anterior) and m. pectoralis major). The IVIM perfusion parameters were assessed by averaging the trace for each b-value in the region of interest before the fitting. Finally, to study which muscle group is more involved in playing tennis, the absolute value of the differences in fD* between the rest state, forehand, backhand and service strokes were calculated in the deltoid and rotator cuff muscles.
Statistical analysis: P-values comparing the muscles were calculated using one-tailed paired student t-test. The p-value of the differences was calculated using two-tailed two-sample student t-test.
RESULTS
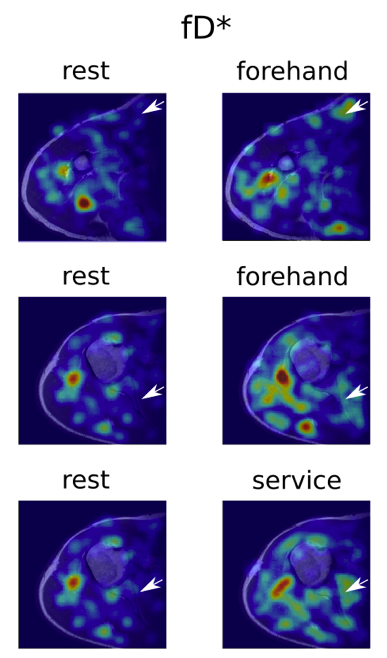
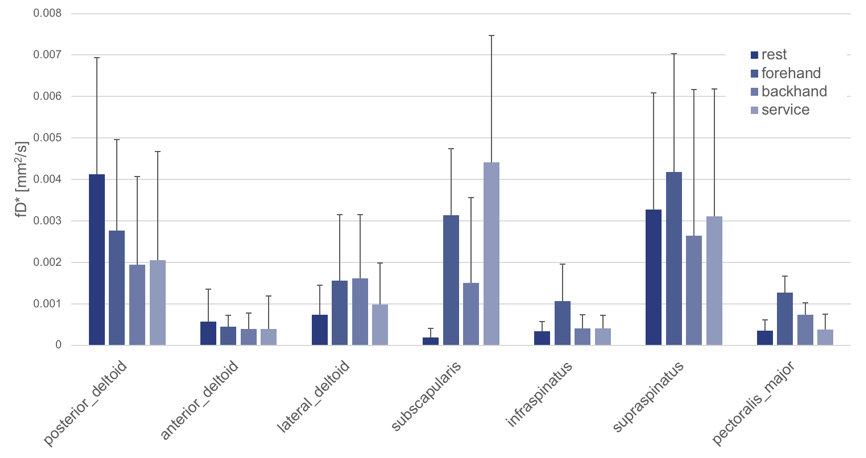
We found significant higher perfusion of the m. subscapularis (3.1±1.6 10-3 mm2/s, p = 0.019) and the m. pectoralis major (1.2±0.4 10-3 mm2/s, p = 0.011) after forehand strokes compared to rest state (0.2±0.2 10-3 mm2/s and 0.3±0.3 10-3 mm2/s). (Fig. 3, Fig. 4) We also found a particular increase in the perfusion after the service stroke in the m. subscapularis(4.4±3.1 10-3 mm2/s, p = 0.040) compared to the rest state. No particular trend was visible in the muscles of the deltoid. We found the rotator cuff muscles (m. subscapularis, m. infraspinatus and m. supraspinatus) to be more involved in tennis playing than the deltoid muscles (p = 0.0005). (Fig. 4, Fig. 5)DISCUSSION
In our preliminary results, we detected increased IVIM microvascular perfusion in m. subscapularis for forehand and service strokes and in the m. pectoralis major after forehand stroke. The minor increase of fD* values after backhand strokes could come from the fact that the strokes were performed double-handed, which was decreasing the amount of work performed by the right shoulder (but not necessary of the left shoulder). Generally, the fD* values of the rest state were high, especially for the posterior m. deltoideus and the m. supraspinatus, compared to the values after exercises. A possible reason for the high fD* values could have been prior muscle activation of the volunteers. In order to validate and improve the significance of this work more experiments are needed.CONCLUSION
This work shows how IVIM perfusion imaging offers the possibility to study complex muscle activation upon playing tennis. Better understanding of the pattern of muscle utilization during complex sport motion might help to prevent injuries, improve regeneration and training efficiency of athletes.Acknowledgements
Christian Federau is supported by the Swiss National Science Foundation.References
1. Filli, L., Boss, A., Wurnig, M. C., Kenkel, D., Andreisek, G., & Guggenberger, R. (2015). Dynamic intravoxel incoherent motion imaging of skeletal muscle at rest and after exercise. NMR in Biomedicine. http://doi.org/10.1002/nbm.32452.
2. Nguyen, A., Ledoux, J. B., Omoumi, P., Becce, F., Forget, J., & Federau, C. (2017). Selective microvascular muscle perfusion imaging in the shoulder with intravoxel incoherent motion (IVIM). Magnetic Resonance Imaging. http://doi.org/10.1016/j.mri.2016.08.005
Figures