1328
Diagnostic performance of three-dimensional fast-spin echo(3D MATRIX) accelerated with compressed sensing(CS) for internal injury of the knee1Peking University Third Hospital, Beijing, China
Synopsis
We aimed to evaluate the diagnostic performance of a three-dimensional fast-spin echo(3D MATRIX) accelerated with compressed sensing(CS) for internal injury of the knee joint.Sixty-two knee joints with trauma were examined at 3T MRI system including conventional 2D FSE protocol and 3D MATRIX before arthroscopic operations. Signal-to-noise ratio(SNR), contrast signal-to-noise ratio(CNR) and diagnostic performance were compared between two sequences. We found that 3D MATRIX had significantly higher SNR and CNR, and provided higher sensitivity but lower specificity for diagnosing cartilage injury compared to conventional 2D FSE. And the two sequences had similar diagnostic performance for ACL and meniscus tear.
Introduction
Three-dimensional fast-spin echo(3D FSE) can acquire isotropic and thin-section images without intersection gaps. It reduces partial volume effects and allows to be multiplanar reformatted. The usefulness of 3D FSE has been evaluated in knee joint imaging1-3. Recently, compressed sensing(CS) is used in 3D FSE to reduce the imaging time4,5, but the diagnostic performance of 3D FSE with CS for knee injury is indeterminate. Our study aims to evaluate the diagnostic performance of a 3D FSE sequence(3D MATRIX) accelerated with CS for internal injury of the knee joint.Methods
Sixty-two knee joints in 62 patients with knee trauma were examined at 3.0T MRI system(by United Imaging, Shanghai, China) before arthroscopic operations. Following conventional 2D FSE protocol(sagittal fat-suppressed PDWI and non-fat-suppressed T1WI, coronal and axial fat-suppressed PDWI, total time 7min26sec), a 3D FSE sequence(3D MATRIX) including sagittal fat-suppressed PDWI(5min4sec) was performed. And then orthometric axial, orthometric coronal, oblique sagittal and oblique coronal images were reformatted after 3D MATRIX scanning.
2D FSE and reformatted 3D MATRIX images were independently reviewed by two radiologists. First, signal-to-noise ratio(SNR) and contrast signal-to-noise ratio(CNR) of 2D and 3D sequences were calculated. Then, two radiologists independently diagnosed cartilage injury, anterior cruciate ligament(ACL) tear and meniscus tear. Sensitivity, specificity and accuracy of 2D FSE and 3D MATRIX were calculated with arthroscopy as the reference standard. Finally, for normal ACL conformed by arthroscopy, a subjective anatomic identification score(both the whole length and two ligament bundles of ACL) was performed.
Paired t-test was used to compare SNR and CNR, McNamer test to compare diagnostic performance for cartilage injury, ACL tear and meniscus tear and Wilcoxon test to analyse difference of ACL anatomic identification scores between two sequences. A p-value less than 0.05 was considered to represent a statistically significant difference.
Results
3D MATRIX had significantly higher(P<0.01) SNR and CNR than the conventional 2D FSE. Twenty-one ACL tear, 51 meniscus tear and 113 cartilage injury were detected by arthroscopic operations. 3D MATRIX had significantly higher sensitivity(70.8% vs. 59.2%, P<0.01) but lower specificity(75.5% vs. 84.2%, P<0.01) than 2D FSE for the evaluation of articular injury, and there were no significant differences in sensitivity, specificity and accuracy between two sequences for diagnosing ACL tear and meniscus tear. For the anatomic identification score of normal ACL, reformatted oblique sagittal images of 3D MATRIX had higher scores to identify whole-length ACL than sagittal images of 2D FSE, and oblique coronal images of 3D MATRIX had higher scores to identify two ligament bundles of ACL than coronal images of 2D FSE.Discussion
In this study, we apply compressed sensing to 3D FSE sequence to reduce the image time. Our study indicates that 3D MATRIX has higher SNR and CNR than 2D FSE. In theory, higher SNR and CNR have potential advantage to reveal damaged tissue.
In our study, 3D MATRIX has higher sensitivity for diagnosing cartilages injury, because the thin-section images provide higher spatial resolution and reduces partial volume effects. This will be beneficial to display small defect of cartilage(Fig.1). However, because 3D FSE sequence has lower intra-section resolution and CS can decrease clarity of cartilage5, 3D MATRIX has a lower specificity for diagnosing cartilage injury. Another important reason is that arthroscopy fails to show subsurface injury, but MR is sensitive to change of subsurface signal(Fig. 2). In addition, our study indicates the two sequences have a similar performance to diagnose ACL and meniscus tear.
As we know, because its oblique course, it’s difficult to identify the complete ACL on a single image of orthometric sagittal view. In this study, because oblique sagittal and coronal view the oblique course of ACL, oblique sagittal image of 3D MATRIX is superior to sagittal image of 2D FSE for identification of whole-length ACL(Fig.3), and oblique coronal image of 3D MATRIX is superior to coronal image of 2D FSE for identification of two ligament bundles of ACL(Fig.4).
Conclutions
3D MATRIX has significantly higher SNR and CNR than 2D FSE. And it provides higher sensitivity but lower specificity for diagnosing cartilage injury compared to conventional 2D FSE. However, the two sequences have similar sensitivity, specificity and accuracy for diagnosing ACL and meniscus tear. The anatomic identification scores of ACL on multiplanar reformatted 3D MATRIX are superior to those on 2D FSE.Acknowledgements
No acknowledgement found.References
1. Ai T, Zhang W, Priddy NK, Li X. Diagnostic performance of CUBE MRI sequences of the knee compared with conventional MRI. CLIN RADIOL. 2012 2012-12-01;67(12):e58-63.
2. Kijowski R, Davis KW, Woods MA, et al. Knee joint: comprehensive assessment with 3D isotropic resolution fast spin-echo MR imaging--diagnostic performance compared with that of conventional MR imaging at 3.0 T. RADIOLOGY. 2009 2009-08-01;252(2):486-95
.3. Kudo H, Inaoka T, Kitamura N, et al. Clinical value of routine use of thin-section 3D MRI using 3D FSE sequences with a variable flip angle technique for internal derangements of the knee joint at 3T. MAGN RESON IMAGING. 2013 2013-10-01;31(8):1309-17.
4. Henninger B, Raithel E, Kranewitter C, Steurer M, Jaschke W, Kremser C. Evaluation of an accelerated 3D SPACE sequence with compressed sensing and free-stop scan mode for imaging of the knee. EUR J RADIOL. 2018 2018-05-01;102:74-82.
5. Kijowski R, Rosas H, Samsonov A, King K, Peters R, Liu F. Knee imaging: Rapid three-dimensional fast spin-echo using compressed sensing. J MAGN RESON IMAGING. 2017 2017-06-01;45(6):1712-22.
Figures
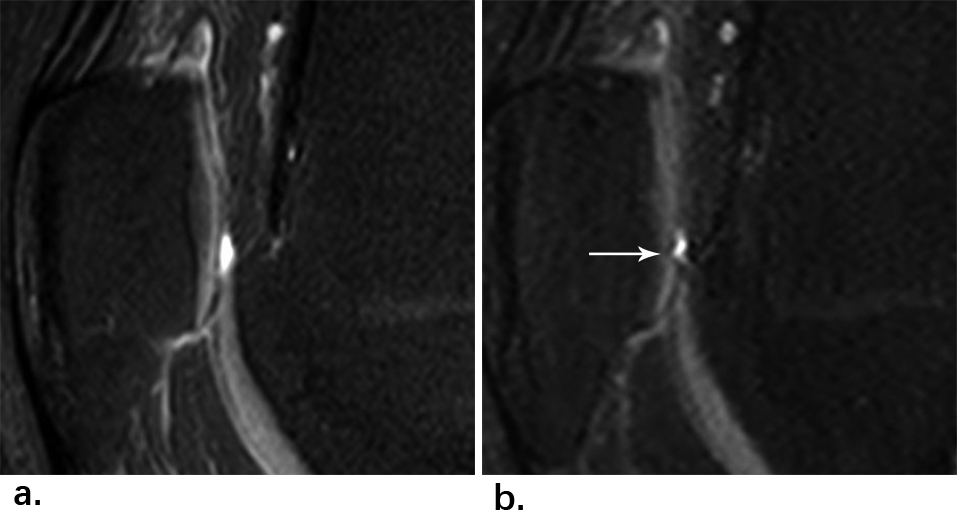
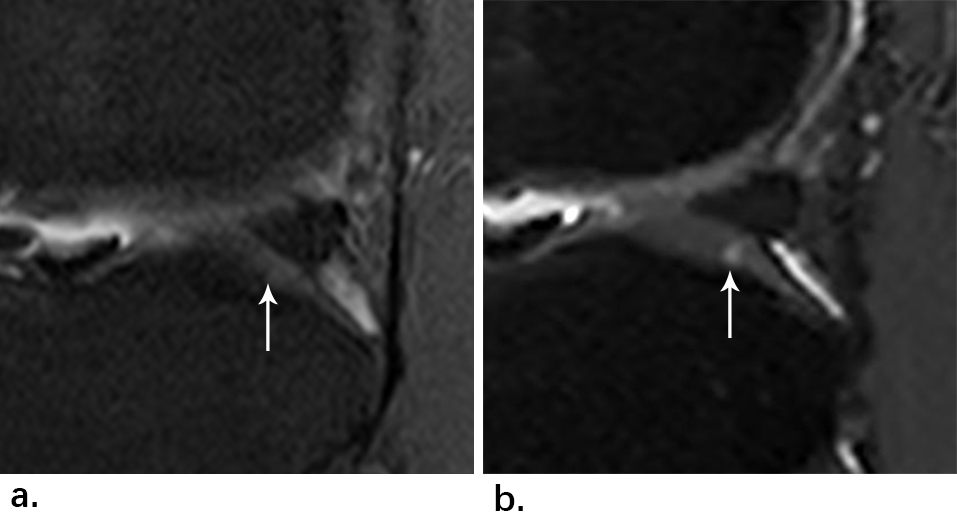
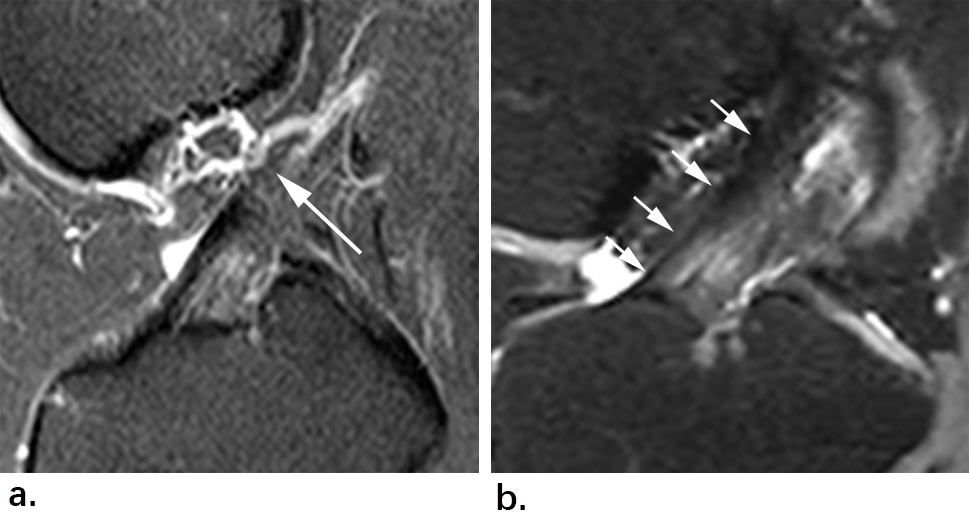
Fig. 3 MR images of a 17-year-old woman with normal ACL. (a)Sagittal fat-suppressed PDWI of 2D FSE can’t show the complete ACL in a single section and partial ligament near femur(arrow) is invisible. However, (b) reformatted oblique sagittal fat-suppressed PDWI of 3D MATRIX can show clearly the whole-length ACL(arrow) in a single section.
Note: ACL - anterior cruciate ligament.
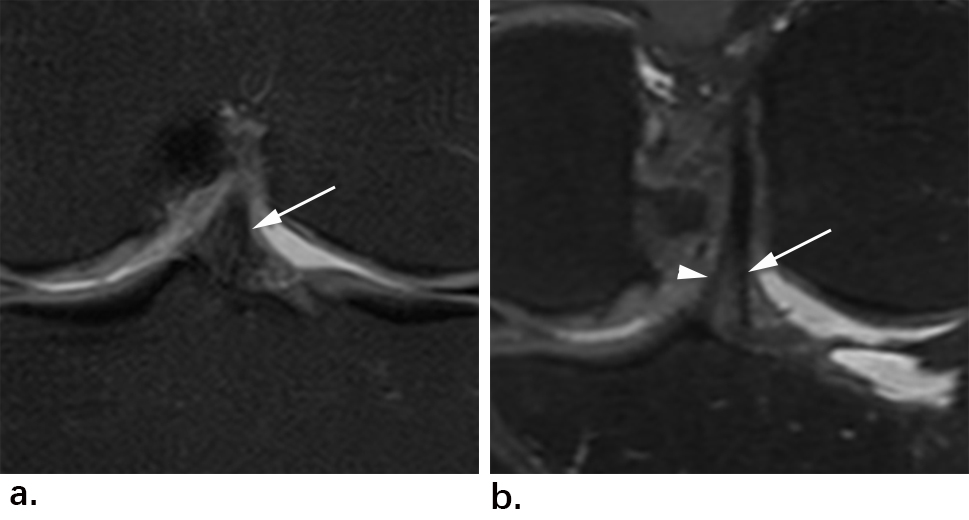
Fig. 4 MR images of a 48-year-old man with normal ACL. (a)Coronal fat-suppressed PDWI of 2D FSE shows normal ACL(arrow), but it’s difficult to identify the two ligament bundles(AMB and PLB). (b) Reformatted oblique coronal fat-suppressed PDWI of 3D MATRIX can identify clearly AMB(triangle) and PLB(arrow).
Note: ACL - anterior cruciate ligament; AMB - anteromedial bundle; PLB - posterolateral bundle.