1326
Simultaneous image super-resolution and contrast synthesis techniques applied to routine clinical magnetic resonance images of the knee for advanced automated processing of joint cartilageAles Neubert1, Pierrick Bourgeat1, Jose Manjon2, Craig Engstrom3, Shekhar S Chandra3, Stuart Crozier3, and Jurgen Fripp1
1AeHRC, CSIRO, Brisbane, Australia, 2ITACA institute, Universidad Politécnica de Valencia, Valencia, Spain, 3University of Queensland, Brisbane, Australia
Synopsis
While high resolution 3D MR images are well suited for automated cartilage segmentation in the human knee joint, they are not routinely acquired in clinical practice which limits opportunities for reliable segmentation of cartilage using automated algorithms. We propose a neural network for generating synthetic MR images with enhanced contrast and higher spatial resolution from routine, low resolution clinical knee scans. Segmentation results showed that accurate cartilage segmentation can be obtained using the synthesised images.
Introduction
While high resolution 3D magnetic resonance (MR) images are well suited for automated cartilage segmentation in the human knee joint, they are not routinely acquired in clinical practice, which limits opportunities for reliable segmentation of cartilage using automated algorithms. In this work, we propose a neural network for generating synthetic MR images with enhanced contrast and higher spatial resolution from routine, low resolution clinical knee scans. To evaluate the clinical utility of the synthetic images, we performed the cartilage segmentation on both the high resolution images and the synthesised ones, and compared their performance in terms of Dice score with the manual segmentations.Methods
Data used in this study were obtained from the OAI database. 796 pairs of sagittal 3D DESS with water excitation (in-plane 0.37x0.37mm, slice thickness 0.7mm) and sagittal intermediate weighted 2D TSE with fat suppression (in-plane 0.36x0.36mm, slice thickness 3mm) images from the Incidence and Progression cohorts were used for training. An additional 88 pairs with expert manual segmentations on the DESS from the Progression cohort and were used as the testing dataset. All TSE images where rigidly aligned to their corresponding DESS and resampled to DESS resolution using BSpline. The synthesis was performed using patches. Each patch of size 11×15×15 voxels on the TSE was used to estimate a patch of size 1×3×3 voxels on the DESS. The voxels values of the TSE patch were used as input to a feed-forward, fully connected neural network with 3 layers with 800, 200 and 50 neurons, respectively (Fig. 1). The activation function was a rectified linear and the loss function was set to mean square error (MSE) between the generated patch and the target patch. The network was trained using stochastic gradient descent optimisation with batches of size 50. The training set was split (80/20) for training and validation. Both the original 3D DESS, synthesised 3D DESS and resampled 2D TSE from the testing set were then segmented using a statistical shape model based method1, and their cartilage segmentations compared to the manual segmentation in terms of Dice score.Results
The median Dice score in tibial cartilage was 0.78 for the DESS, 0.74 for the synthesised DESS and 0.60 for the TSE. The median Dice score in femoral cartilage was 0.81 for the DESS, 0.77 for the synthesised DESS and 0.70 for the TSE. Boxplots for both cartilages are in Fig 2. Representative example of the synthesised DESS and corresponding cartilage segmentation is presented in Fig 3.Discussion
Segmentation results showed that the cartilages extracted from the synthetic data had much higher Dice score than the ones obtained from the original 2D TSE, and were closer to the ones obtained from the 3D DESS. It could be argued that the segmentation could be performed directly using the neural network, but one major advantage of learning the contrast synthesis instead of direct segmentation it that the training only requires pairs of images using the 2 contrast, and does not require manual segmentations for both contrasts. Therefore, the method can easily be extended to more contrast.Conclusion
We have presented a method for generating synthetic 3D DESS images with high resolution and contrast characteristics from routine, lower resolution 2D TSE images of the knee joint. Results show that accurate segmentation results can be obtained from the synthesised images.Acknowledgements
No acknowledgement found.References
1. Fripp J, Crozier S, Warfield SK, Ourselin S. Automatic segmentation and quantitative analysis of the articular cartilages from magnetic resonance images of the knee. IEEE transactions on medical imaging 2010 1;29(1):55–64Figures
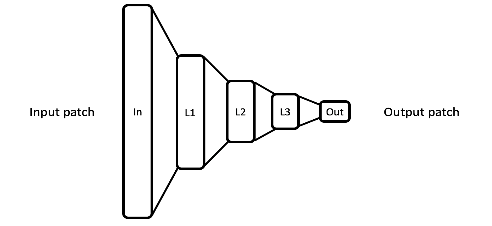
Figure
1: Architecture of the proposed network.

Figure 2: DESS
(left), synthesised DESS (middle), and TSE (right) and their
segmentations (manual for the DESS, automated for synthesised DESS
and TSE). The synthesised image is able to reduce the chemical shift
artefact in TSE scans that normally leads to a visually thinner
cartilage (arrow A), which helps to improve the automated
segmentation (thicker cartilage at arrow A, non-missing cartilage at
arrow B, corrected segmentation at arrow C).

Figure
3: Dice score for the segmentation results on the DESS, synthetic
DESS and TSE scans for femoral and tibial cartilage plates.