1311
Quantitative Articular Cartilage Assessment in Patients with Juvenile Osteochondritis Dissecans (JOCD) at 3T MRI1Center for Magnetic Resonance Research (CMRR), University of Minnesota, Minneapolis, MN, United States, 2Radiology, University of Minnesota, Minneapolis, MN, United States, 3Orthopaedic Surgery, University of Minnesota, Minneapolis, MN, United States, 4Veterinary Clinical Sciences, University of Minnesota, St. Paul, MN, United States
Synopsis
Juvenile osteochondritis dissecans (JOCD) is a disease affecting the knee joint of young active patients that can lead to early osteoarthritic changes. JOCD lesions are formed deep to the articular cartilage with late changes in the overlying articular cartilage. Our study was motivated by clinical observations that the opposing articular cartilage might be affected early. In this study, we observed a significant increase in T2* relaxation times in the articular cartilage of the medial tibia directly opposing the lesions when compared to the control region on the lateral site. These findings might indicate compositional changes in the tibial cartilage matrix due to increased biomechanical loading. Further study of T2* mapping as a potentially clinically realizable method to stage and prognosticate JOCD are warranted.
Purpose
Juvenile osteochondritis dissecans (JOCD) is a disease characterized by the formation of lesions initiating in the sub-articular epiphyseal cartilage and, later, ossifying as the joint develops. The articular cartilage overlying the lesion remains clinically-normal for a long period, and changes are noted clinically only in very late stages of the disease. Current clinical protocols based on qualitative assessments cannot detect whether the intact overlying articular cartilage is injured. Thus, it is of potential clinical interest to non-invasively evaluate the health of the femoral and tibial articular cartilage in the vicinity of the JOCD lesion. Our interest in these location was motivated by arthroscopic observations noted by orthopaedic surgeons in subtle changes of the opposing tibial articular surface. It has been previously shown that T2 and T2* relaxation times can quantitative measure cartilage integrity in JOCD [1,2]. The purpose of this study was to investigate whether T2* relaxation times are altered in the articular cartilage of the distal femur (adjacent to JOCD lesions) and proximal tibial (opposing the JOCD lesions) compared to cartilage on the opposite side of the joint.Methods
Subjects. The institutional review board approved all procedures. Eight patients with suspected JOCD (6M/2F; average age = 14.0 years; range: 11-19 years) were enrolled.
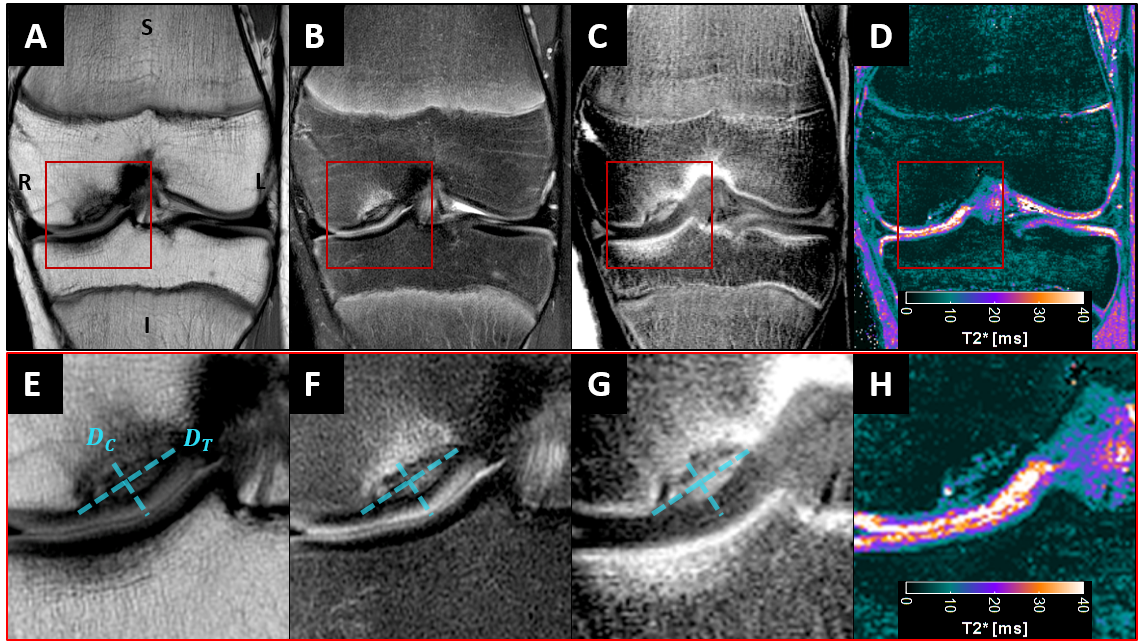
Imaging. MRI data was acquired on a 3T Magnetom Prisma MRI system (Siemens Medical Systems) with a 15-channel transmit/receive knee RF coil. Clinical T1-weighted, T2-weighted, and PD-weighted images were collected in three orthogonal planes. A gradient-recalled-echo T2* mapping sequence (TR/TE/ΔTE = 1150/2.63/2.96 ms, 6 echoes, matrix = 352×352, resolution = 0.43×0.43, slice thickness/gap = 2.0/0.0 mm, 39 slices, flip angle = 60°, voxel bandwidth = 395-405 Hz, and acquisition time = 6min:57sec) was acquired. All lesions were radiologically classified as stable lesions without obvious articular cartilage fissures or defects.
Analysis.
T2* maps: Articular cartilage T2* relaxation time maps were fit from the six measured TEs on a voxel-wise basis. For segmentation, the final three echo images of the T2* mapping sequence were averaged to enhance the cartilage-to-bone contrast. The cartilage tissue was segmented semi-automatically using ITK-SNAP [3]. Region-of-interests (ROIs) for T2* measurements were defined from the segmented cartilage masks as shown in Figure 1.
Statistics: We hypothesized that T2* relaxation times are altered in: (i) the central aspect of the medial femoral condyle (MFCC) vs. the lateral femoral condyle (LFCC); and (ii) the medial tibia (MTC) vs. the lateral tibia (LTC). These hypotheses were tested using a Wilcoxon-rank-sum test with p<0.05 considered statistically significant.
Results
All lesions occurred on the central aspect of the medial femoral condyle (MFCC). No macroscopic abnormalities of the femoral or tibial articular cartilage were observed in any of the knees. Cartilage depth and parent bone edges were clearly visible on clinical PD- or T2-weighted images and T2*-first-echo images, respectively, as shown in Figure 2. Cartilage T2* values for all subjects are shown in Table 1. The MFCC had increased T2* values compared to the same location on the lateral femoral condyle (LFCC) (26.4 ± 4.4 ms vs. 23.1 ± 3.0 ms; p=0.090), though not statistically significant. The opposing articular cartilage on the medial tibia (MTC) had significantly increased T2* values compared to the lateral tibia (LTC) (18.8 ± 2.8 ms vs. 15.8 ± 2.5 ms; p=0.029).Discussion
We observed a significant increase in T2* relaxation times in the articular cartilage of the medial tibia directly opposing the lesions compared to the lateral tibia. In contrast, there was no significant difference in T2* relaxation times noted in the articular cartilage of the medial femur immediately superficial to the lesion compared to the lateral femur. Our results in the femur are consistent with a prior study of JOCD patients that found no T2 differences in the cartilage overlying the JOCD lesion versus cartilage adjacent to the lesion nor in the cartilage adjacent to the lesion versus cartilage in controls [2]. No prior reports have assessed the tibial articular cartilage opposing the lesions. Our tibial findings may relate to compositional changes in the tibial cartilage matrix due to abnormal contact with the femoral cartilage lesion site. These findings are considered to be preliminary due to the low number of patients included in the study and motivate further study of T2* mapping as a potentially clinically-realizable method to stage and prognosticate JOCD.Acknowledgements
This study was supported by the NIH (R01AR070020, K01AR070894, and P41EB015894) and the W. M. Keck Foundation.References
1. Ellermann J, Johnson CP, Wang L, Macalena JA, Nelson BJ, LaPrade R. Insights into the Epiphyseal Cartilage Origin and Subsequent Osseous Manifestation of Juvenile Osteochondritis Dissecans with a Modified Clinical MR Imaging Protocol: A Pilot Study. Radiology. 2017;282:798-806
2. Nguyen JC, Liu F, Blankenbaker DG, Woo KM, Kijowski R. Juvenile Osteochondritis Dissecans: Cartilage T2 Mapping of Stable Medial Femoral Condyle Lesions. Radiology. 2018; 288:536–543
3. Yushkevich PA, Piven J, Hazlett HC, Smith RG, Ho S, Gee JC, and Gerig G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116-28
Figures