1295
Trabecular Bone Imaging Using a 3D Adiabatic Inversion Recovery Prepared Ultrashort Echo Time Cones (3D IR-UTE Cones) Sequence1Radiology, University of California, San Diego, San Diego, CA, United States, 2GE health care, San Diego, CA, United States, 3VA San Diego Healthcare System, San Diego, CA, United States
Synopsis
The trabecular bone is both functionally and biomechanically important for vertebrates, including humans. Evaluation of trabecular bone provides important information about risk of both osteoporosis and bone fracture. Direct MR imaging of trabecular bone is difficult due to its ultrashort T2* and low water content, resulting in little or no signal when conventional pulse sequences are used. The purpose of this study was to develop and evaluate a 3D adiabatic inversion recovery prepared UTE Cones (3D IR-UTE-Cones) sequence for volumetric imaging of trabecular bone ex vivo and in vivo on a clinical 3T scanner in clinically acceptable scan times.
Introduction
Areal bone mineral density (BMD) of trabecular bone in the spine and/or hip is the most commonly used clinical diagnostic test for assessing skeletal status and fracture risk. More recently, computed tomography (CT) and dual energy X-ray absorptiometry (DEXA) have provided quantitative analysis through measurement of volumetric BMD. MRI is routinely used in the diagnosis of soft tissue disease. However, bone is “invisible” when using clinical sequences due to bone’s ultrashort T2* (between 0.2 to 0.6 ms) 1. Ultrashort Echo Time (UTE) sequences with TEs less than 100 µs have been developed, making direct detection of signal from bone possible 2. In this study, we report a 3D adiabatic inversion recovery prepared UTE Cones (3D IR-UTE-Cones) sequence for high contrast direct imaging of trabecular bone on a clinical 3T scanner, with full suppression of the surrounding long T2 tissues, including the bone marrow and muscle.Methods
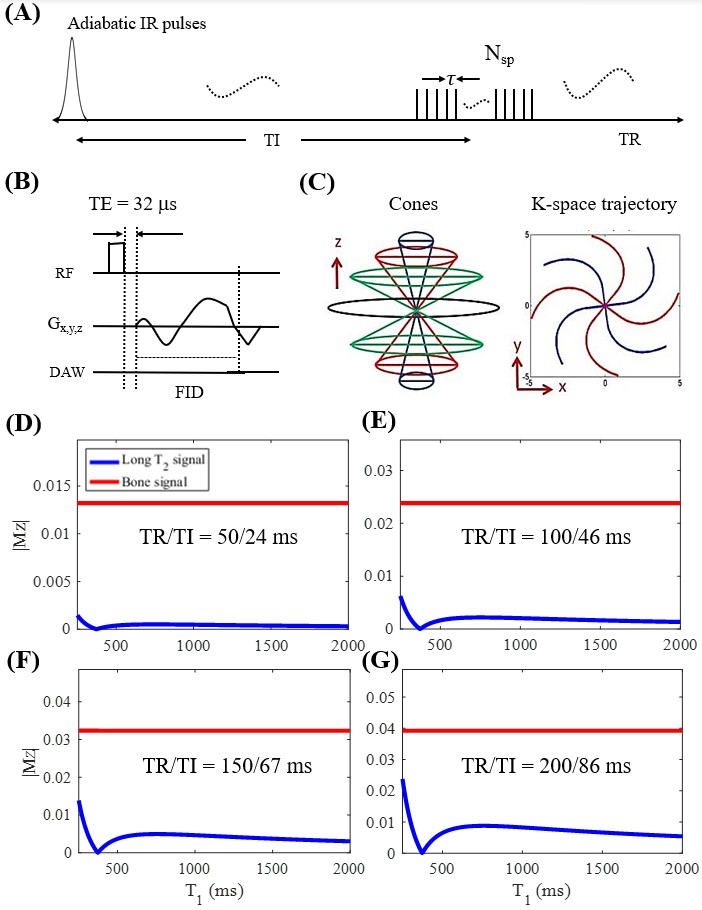
Since marrow fat is abundant in trabecular bone, direct imaging of trabecular bone requires efficient suppression of signals from marrow fat. Adiabatic inversion pulse provides uniform inversion of long T2 tissues, such as marrow fat and muscle, while saturating ultrashort T2 tissues, such as cortical and trabecular bone, which can be subsequently detected with UTE acquisitions. Meanwhile, marrow fat in trabecular bone is subject to strong susceptibility and has a broad range of resonance-frequencies. For more robust suppression of marrow fat, we proposed a novel technique employing an adiabatic inversion pulse with a relatively broad spectral bandwidth to robustly invert and null the longitudinal magnetizations of marrow fat, followed by highly time-efficient 3D UTE Cones sampling 3,4. To improve the acquisition efficiency, a series of spokes (Nsp) were acquired after each IR pulse (Figure 1A). For each spoke, a short rectangular pulse (e.g., 72 µs) was used for non-selective signal excitation (Figure 1B), then followed by a Cones data acquisition (Figure 1C). More efficient long T2 (i.e. marrow fat and muscle) suppression can be achieved with a shorter TR. Bloch simulation was performed for four different TRs (i.e., 50, 100, 150 and 200ms) with corresponding best TIs in order to evaluate the effectiveness of long T2 suppression. The optimal TI was determined, similar to previous studies, with nulling T1 from 350-400 ms 3,5. The T1 of trabecular bone was set to 150 ms and water proton density was set to 10% in simulation.
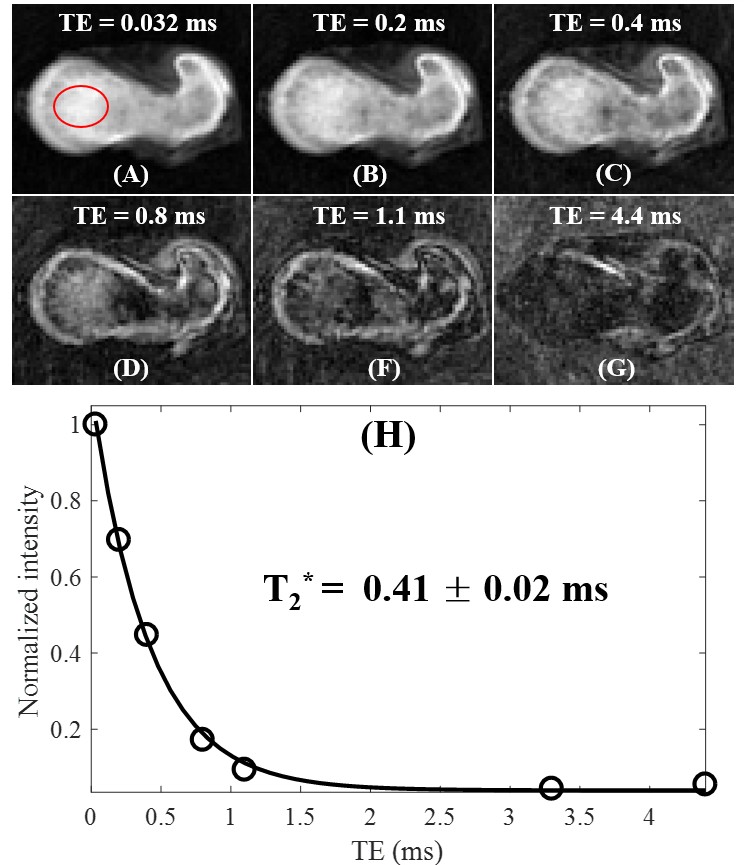
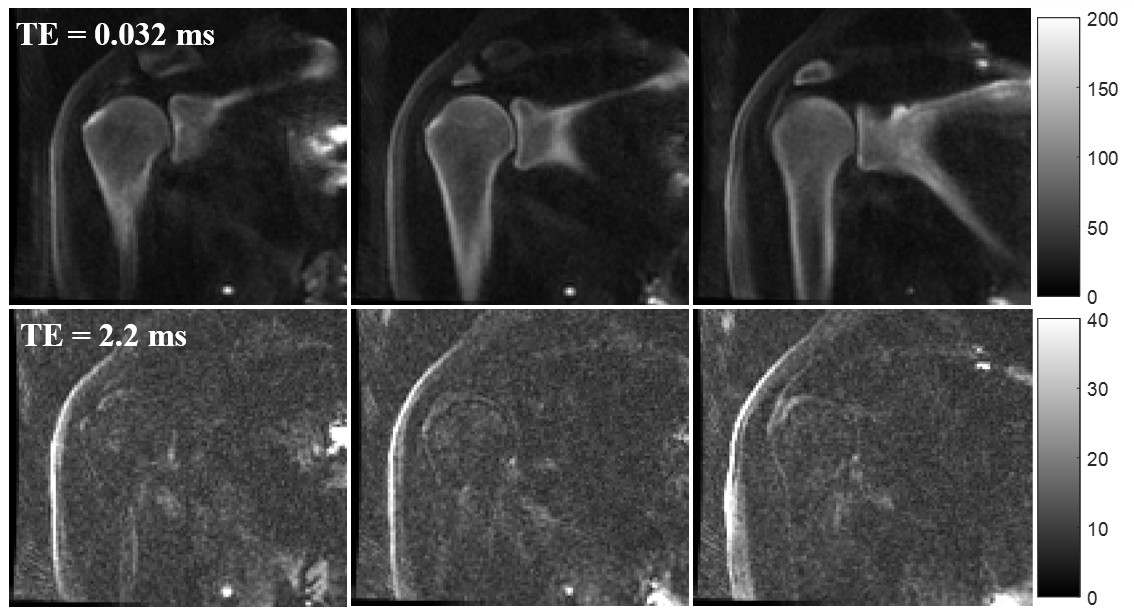
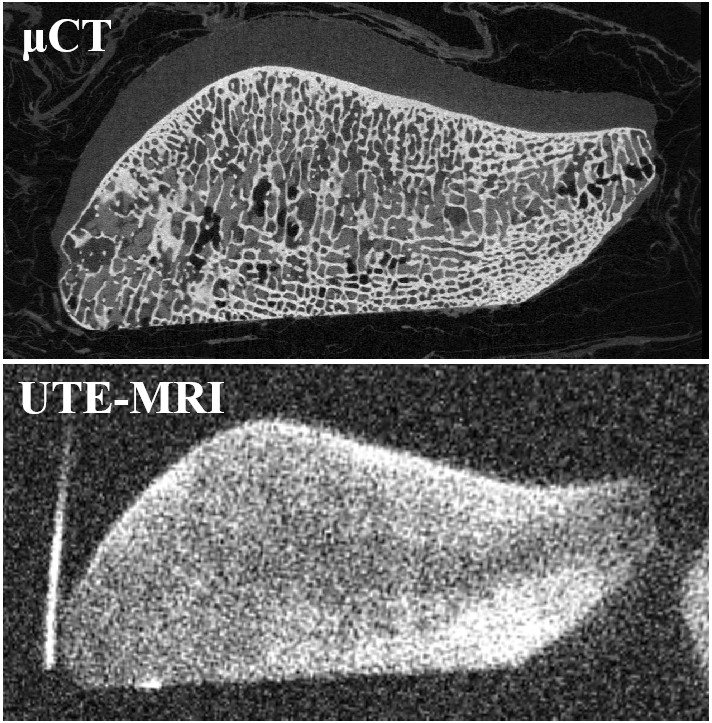
Ex vivo imaging was performed for hip, patellar, and shoulder trabecular bone samples. Quantitative 3D IR-UTE-Cones was employed for bound water T2* measurement of the hip bone sample (TE=0.032,0.2,0.4,0.8,1.1,3.3 and 4.4ms; TR/TI=82/38ms). Dual-echo IR-UTE-Cones was used for shoulder bone imaging with TE=0.032/2.2ms and TR/TI=88/40ms. The small patellar sample was imaged with a high-resolution IR-UTE-Cones sequence (voxel size=156×156×300µm3, TR/TI=133/58ms) using a 30mL birdcage coil. The signal intensity of the patellar sample was also compared with the corresponding μCT (18×18×18µm3) images. Then, in vivo spine and hip bone imaging was performed in a coronal scan on two volunteers (male, 36 and 37 years old) following IRB approval with written informed consent. The sequence parameters of IR-UTE-Cones sequence are shown as follows: FOV=45×45×20.8cm3, matrix=180×180×52, TR/TI=183/78 ms, flip angle=25°, Nsp=5, spoke interval =6ms, sampling BW=166kHz, IR pulse bandwidth=1.64 kHz, scan time=10 min.
Results and Discussion
Figures 1D-F show the simulation results of signal suppression for the long T2 tissues with a broad range of T1s (i.e., from 250 to 2000 ms) using the IR sequence. The results demonstrate that a shorter TR leads to better long T2 suppression. Even with a relatively long TR of 200ms, our results still show that bone signal is at least four times higher than that of long T2 tissues.
Figure 2 shows selective IR-UTE-Cones images of the femur sample with different echo times. Excellent T2* fitting was achieved for the trabecular bone region with a T2* of 0.41±0.02ms. Figure 3 shows dual-echo images of the shoulder sample. The second echo shows almost no signals inside of the trabecular bone, which demonstrates excellent suppression of marrow fat.
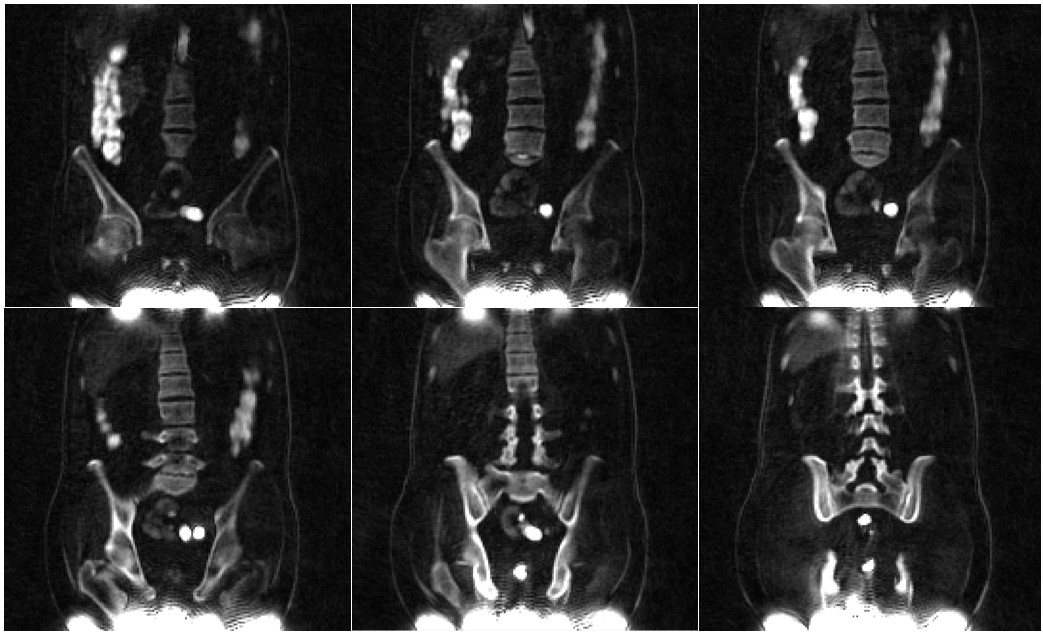
The comparison between IR-UTE-Cones imaging and μCT imaging is shown in Figure 4. The signal intensity distributions in both images are quite similar, suggesting that trabecular bone is being selectively imaged with the IR-UTE-Cones sequence. High contrast imaging of trabecular bone in the spine and hip of a volunteer using the 3D IR-UTE-Cones sequence is shown in Figure 5, demonstrating the clinical feasibility of this technique for direct imaging of trabecular bone in vivo.
Conclusion
The 3D IR-UTE-Cones sequence can be used for high contrast direct imaging of trabecular bone with excellent suppression of long T2 tissues. This technique may be used to provide information on bone quality and risk of bone fracture in subjects with osteoporosis.Acknowledgements
The authors acknowledge grant support from GE Healthcare, NIH (1R21AR073496, R01AR068987), and the VA Clinical Science and Rehabilitation R&D Awards (I01CX001388 and I01RX002604)References
1. Du J, Carl M, Bydder M, Takahashi A, Chung CB, Bydder GM. Qualitative and quantitative ultrashort echo time (UTE) imaging of cortical bone. J Magn Reson 2010;207(2):304-11.
2. Robson MD, Gatehouse PD, Bydder M, Bydder GM. Magnetic resonance: an introduction to ultrashort TE (UTE) imaging. J Comput Assist Tomogr 2003;27:825-846.
3. Carl M, Bydder GM, Du J. UTE imaging with simultaneous water and fat signal suppression using a time-efficient multispoke inversion recovery pulse sequence. Magn Reson Med 2016;76:577–582.
4. Larson PE, Conolly SM, Pauly JM, Nishimura DG. Using adiabatic inversion pulses for long-T2 suppression in ultrashort echo time (UTE) imaging. Magn Reson Med 2007; 58:952-961.
5. Ma YJ, Zhu Y, Lu X, Carl M, Chang EY, Du J. Short T2 imaging using a 3D double adiabatic inversion recovery prepared ultrashort echo time cones (3D DIR-UTE-Cones) sequence. Magn Reson Med 2018;79(5):2555-63.
Figures