1293
Prevalence and Clinical Significance of Residual or Reconverted Red Bone Marrow on Knee MRI in Young Adults1Menzies Institute for Medical Research, University of Tasmania, Hobart, Australia, 2Epidemiology and Preventive Medicine, Monash University, Melbourne, Australia, 3Institute of Bone and Joint Research, University of Sydney, Sydney, Australia, 4Murdoch Childrens Research Institute, Melbourne, Australia, 5Radiology, Royal Hobart Hospital, Hobart, Australia
Synopsis
An abnormal distribution of residual or reconverted red bone marrow (RBM) has been identified on routine knee MRI. We aimed to identify the prevalence and the association between RBM and symptoms and structural abnormalities in a young population (n=327, aged 31-41 years). The presence of RBM in the distal femoral, proximal tibial and fibular metaphysis was graded based on the percentage of the metaphysis occupied (grade 0 to 3). Reconverted or residual RBM around the knee joint was present only among females and always involved the distal femoral region. RBM was associated with overweight measures and knee joint pain.
Introduction
An abnormal distribution of residual or reconverted red bone marrow (RBM) has been identified on routine knee magnetic resonance imaging (MRI); however, the clinical significance of these marrow changes is still unclear. The prevalence of the RBM, the patterns of distribution of the RBM within the knee joint, and the association with clinical symptoms and joint structural abnormalities has not been studied in young adults. We aimed to identify the prevalence and pattern of distribution of residual or reconverted RBM on knee MRI, and the association between residual or reconverted RBM, and clinical symptoms and joint structural abnormalities in young adults.Methods
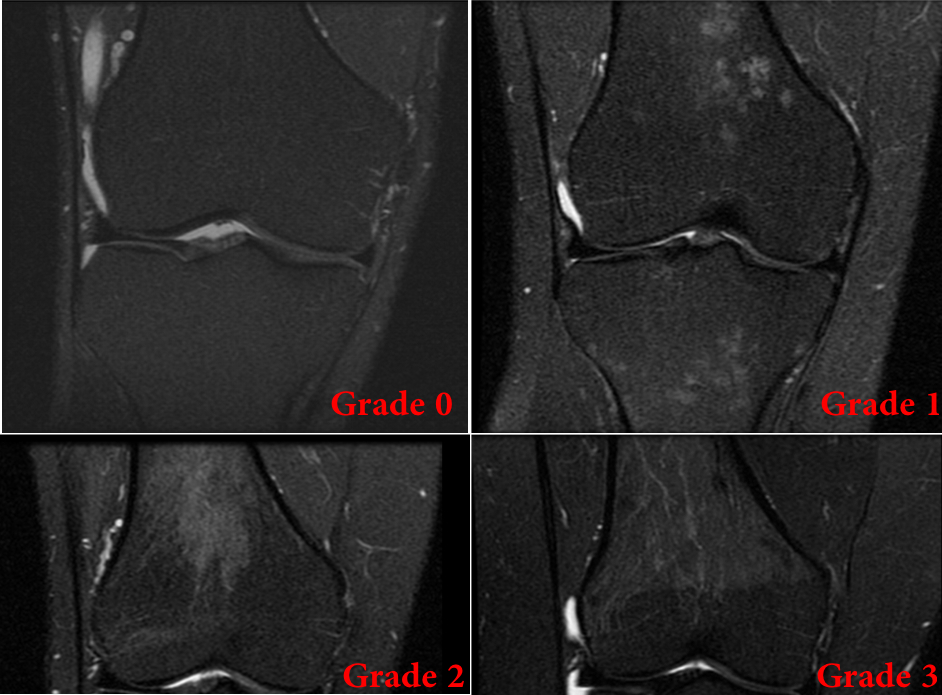
Participants broadly representative of the Australian population (n=327, aged 31-41 years) were selected from the Childhood Determinants of Adult Health (CDAH) Study1. CDAH study is a follow-up study of the Australian Schools Health and Fitness (ASHFS) Survey conducted in school kids of the age of 7-15 years in 1985. Participants’ weight, height and physical activity measures were assessed in the CDAH study. After 4 - 5 years, they underwent T1-weighted fat-suppressed and proton density-weighted fat-suppressed MRI scans of their knee. Knee symptoms were assessed using Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) questionnaires. Cartilage defects, bone marrow lesions (BMLs), meniscal tears and meniscal extrusions were measured from MRI using semi-quantitative scoring systems (modified Outerbridge classification system and WORMS system). The presence of RBM in the distal femoral, proximal tibial and fibular metaphysis was recorded, and the distribution of RBM in the femur and tibia was further graded based on the percentage of the metaphysis occupied (grade 0 = no lesion, grade 1 = <30%, grade 2 = 30-60%, and grade 3 = >60%; Figure 1)2. Presence of any residual or reconverted RBM was defined as grade >1. Log binomial regressions were used to describe the associations between the presence of RBM and lifestyle factors, clinical symptoms and structural abnormalities of the knee joint.Results
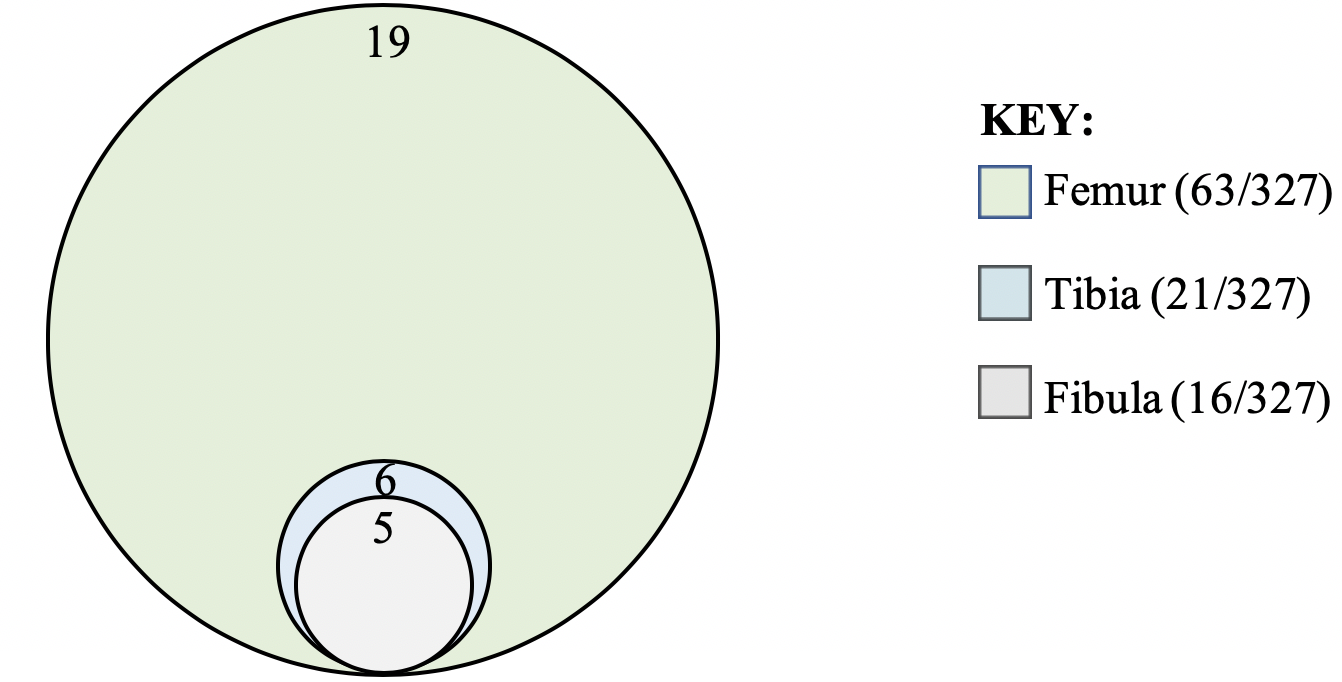
Residual or reconverted RBM was observed on a total of 63 out of 327 participants (grade 1 = 10.4%, grade 2 = 7% and grade 3 = 1.8%). No participants had tibial or fibular involvement in the absence of femoral residual or reconverted RBM (Figure 2). Residual or reconverted RBM was prevalent only amongst females. Presence of residual or reconverted RBM was associated with increased weight (PR 1.03/kg, 95% CI 1.01 to 1.06), BMI (PR 1.09/kg/m2, 95% CI 1.03 to 1.16) and overweight status (PR 2.19, 95% CI 1.07 to 4.51). There was no significant association between the presence of RBM and age, smoking status or physical activity levels. Residual or reconverted RBM was associated with WOMAC knee pain (PR 2.33, 95% CI 1.13 to 4.81) after adjusting for age, BMI and injury status. Higher grades of RBM were associated with higher knee pain (Figure 3). There was no association between residual or reconverted RBM and knee cartilage defects, subchondral BMLs or meniscal lesions.Discussion
This is the largest sample size study to explore the correlates of residual or reconverted RBM around knee joint in a population based sample. Higher prevalence of reconverted or residual RBM around the knee joint among females has been reported previously2,3 and we found that they were only among females. We did not find an association with age although RBMs are mostly reported in young adults. This could be due to the short range of age (31-41 years) of the study sample. No previous studies have explored the pattern of RBM around knee joint and we found that the RBMs always involved the distal femoral region. We also found that residual or reconverted RBM was associated with overweight measures as reported in the previous smaller sample size studies3. Most importantly, we found that RBM was associated with knee symptoms such as WOMAC knee pain independent of BMI, age and injury status. Further longitudinal studies are warranted to explore the potential of RBM to cause knee joint pain without influencing the joint structural abnormalities.Conclusion
Reconverted or residual RBM around the knee joint was present only among females and always involved the distal femoral region. Residual or reconverted RBM was associated with overweight measures and knee joint pain.Acknowledgements
Special thanks go to the National Health and Medical Research Council of Australia (NHMRC) for funding CDAH Knee Study. The roles of Liz O’Loughlin and Judy Hankin in collecting the data, Marita Dalton in managing the database and the participants who made this study possible are gratefully acknowledged. B Antony is supported by the NHMRC Early Career Postdoctoral Clinical Research Fellowship and Farrell Family Senior Research Fellowship.References
1. Antony B, Jones G, Venn A, et al. Childhood Physical Performance Measures and Adulthood Knee Cartilage Volume and Bone Area: A 25-Year Cohort Study. Arthritis Care Res (Hoboken). 2015;67(9):1263-71.
2. Arslan G, Ozmen E, Soyturk M. MRI of Residual Red Bone Marrow in the Distal Femur of Healthy Subjects. Polish journal of radiology. 2015;80:300-4.
3. Wilson AJ, Hodge JC, Pilgram TK, et al. Prevalence of red marrow around the knee joint in adults as demonstrated on magnetic resonance imaging. Academic radiology. 1996;3(7):550-5.
Figures