1291
Diffusion-Weighted MRI in Juvenile Osteochondritis Dissecans (JOCD) at 3T1Center for Magnetic Resonance Research (CMRR), University of Minnesota, Minneapolis, MN, United States, 2Radiology, University of Minnesota, Minneapolis, MN, United States, 3Orthopaedic Surgery, University of Minnesota, Minneapolis, MN, United States, 4Veterinary Clinical Sciences, University of Minnesota, St. Paul, MN, United States
Synopsis
Diffusion-weighted MRI (DWI) may help elucidate the etiology and progression of juvenile osteochondritis dissecans (JOCD) by probing tissue/cellular characteristics of JOCD lesions and the underlying parent bone. In this study, we observed elevated DWI signal and increased apparent diffusion coefficient (ADC) values within and proximal to OCD lesions compared to surrounding bone marrow and control sites. ADC values within the lesion and the parent bone may help distinguish healing from non-healing lesions, thereby improving prognostication of JOCD and clinical decision making.
Purpose
Pediatric skeletal diseases such as juvenile osteochondritis dissecans (JOCD) manifest in the epiphyseal cartilage and adjacent subchondral bone, yet the etiology and progression of JOCD is poorly understood [1]. Diffusion-weighted MRI (DWI) allows for non-invasive evaluation of the molecular motion of water as a marker for tissue and cellular structure and may be an alternative quantitative measure to contrast-based MRI techniques. Previously, increased apparent diffusion coefficient (ADC) values have been measured within the bone marrow of the distal femur after trauma compared to normal marrow [2]. Additionally, DWI has increased sensitivity to detect bone marrow edema compared to proton density(PD)-weighted clinical imaging [3]. The utility of DWI in the understanding of the pathogenesis of JOCD has not been studied previously, but we hypothesize that it may be useful for patient stratification and to predict whether or not lesions will heal. The purpose of this work was to investigate DWI and report quantitative ADC values in JOCD lesions and the surrounding parent bone in patients with knee JOCD. We compared ADC values between the affected femoral epicondyle and the bone marrow in the unaffected femoral epicondyle. This study is important because DWI may have prognostic value by 1) helping to distinguish healing from non-healing JOCD lesions, 2) evaluating the extent of bone marrow edema, and 3) identifying the structural and biochemical composition of the lesions.Methods
Specimens. All procedures were approved by the institutional review board. Eight patients with suspected JOCD (6M/2F; average age = 14.8 y; range: 9-23 y) were enrolled.
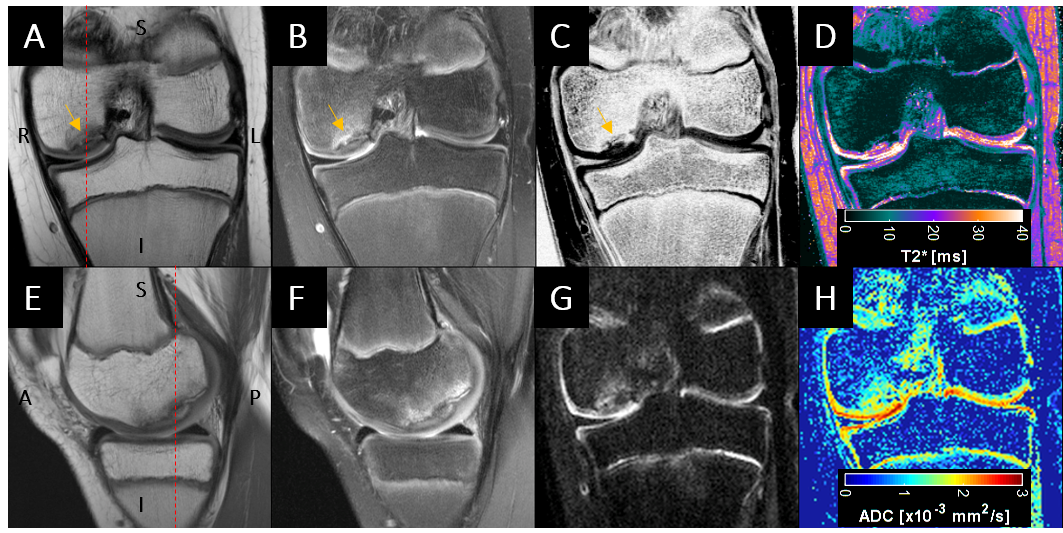
Imaging. MRI data were acquired using a 3T Magnetom Prisma MRI system (Siemens Medical Systems) with a 15-channel transmit/receive knee RF coil. Clinical T1-weighted, T2-weighted, and PD-weighted images were collected in three orthogonal planes. A multi-echo T2* mapping sequence and a segmented, multi-shot DWI sequence were acquired in the coronal plane with the scan parameters listed in Table 1.
Analysis. Apparent diffusion coefficient (ADC) maps were automatically post-processed from DWI images in the Siemens syngo environment. Region of interests (ROIs) were drawn using Matlab (Mathworks) within each condyle of the JOCD-affected and contralateral knee, and median ADC values within the ROIs were measured. To identify ADC values solely at the site of the lesion, the ADC maps were thresholded by the mean ADC value plus two times the standard deviation measured in the contralateral condyle on the OCD-affected knee. Student t-tests were performed to determine statistically-significant differences, defined as p<0.05, in the median ADC values.
Results
OCD lesions were identified in the central aspect of the medial femoral condyle in all patients. No obvious anatomical abnormalities were apparent in the clinical images. Low T2* and ADC values were observed in the medial and lateral epicondyles of the contralateral control knee (Figure 1). In contrast, increased T2* values at or near the location of the lesion were seen in the JOCD-affected knees (Figure 2). Additionally, elevated signal on the DWI images and increased ADC values were detected at and proximal to the location of the lesion. The median ADC values in the lesions (1.53×10-3 ± 0.13 mm2/s) were significantly greater (p<0.001) than the ADC values in the surrounding bone marrow and control sites (Figure 3). The bone marrow adjacent and proximal to the JOCD lesions also had slightly higher ADC values when compared to the same location on the contralateral knee (0.79×10-3 ± 0.14 mm2/s vs. 0.70×10-3 ± 0.08 mm2/s; p=0.078).Discussion
We have demonstrated an increased DWI signal in and around JOCD lesions with measurable ADC values higher than those observed in the contralateral condyle and knee. ADC values in abnormal bone marrow were nearly twice those measured elsewhere [2]. The ADC values in healthy bone marrow reported here are higher than those measured in the bone marrow of healthy adults [3] and in other cancellous bone sites such as the distal femoral neck in older, healthy subjects [4]. The higher ADC values measured here may be a result of increased fatty marrow content in adults, sequences/acquisition parameter differences, or bias from the data fitting operation (e.g. noise thresholding). Future work aims to identify differences in the ADC values over time in JOCD lesions and the surrounding parent bone to correlate with disease progression and stage.Acknowledgements
This study was supported by the NIH (R01AR070020, K01AR070894, P41EB015894, 1S10OD017974-01) and the W. M. Keck Foundation.References
1. Ellermann J, Johnson CP, Wang L, Macalena JA, Nelson BJ, LaPrade R. Insights into the Epiphyseal Cartilage Origin and Subsequent Osseous Manifestation of Juvenile Osteochondritis Dissecans with a Modified Clinical MR Imaging Protocol: A Pilot Study. Radiology. 2017;282:798-806
2. Ward R. Caruthers S, Yablon C, Blake, DiMasi M, Eustace S. Analysis of Diffusion Changes in Posttraumatic Bone Marrow Using Navigator-Corrected Diffusion Gradients. AJR. 2000;174:731-734.
3. Menezes NM, Connolly SA, Shapiro F, Olear EA, Jimenez RM, Zurakowski D, Jaramillo D. Early Ischemia in Growing Piglet Skeleton: MR Diffusion and Perfusion Imaging. Radiology. 2007;242:129-136.
4. Capuani S. Water diffusion in cancellous bone. Micropourous and Mesoporous Materials. 2013;178:34-38.
Figures