1264
Aerobic exercise enhances 31P MRS measured mitochondrial function independent of statin useJill M Slade1, George S Abela2, David M Hurley1, and Ronald A Meyer3
1Radiology, Michigan State University, East Lansing, MI, United States, 2Medicine, Michigan State University, East Lansing, MI, United States, 3Physiology, Michigan State University, East Lansing, MI, United States
Synopsis
Phosphorus MRS is the gold standard measure of in vivo mitochondrial function. In this study, 31P MRS was used to examine exercise-induced adaptations in mitochondrial function in the presence of concurrent statin use. The results show that aerobic exercise training significantly improved muscle oxidative capacity of the plantar flexor muscles in older adults independent of statin use.
Introduction
Statin medications are widely used to reduce cholesterol and more importantly to improve cardiovascular health 1. While important for generally reducing major cardiovascular risk factors and events, there are potential deleterious impacts for statins on skeletal muscle function2. It has been shown that statins reduce skeletal muscle oxidative capacity3,4 and mitochondrial respiration in complex II5 as well as reduce cardiorespiratory and mitochondrial adaptations expected with aerobic exercise training6. However, a recent study in rodents showed robust increases in citrate synthase activity and mitochondrial content following exercise with statin treatment in rats7. The current study evaluated the influence of statin use on exercise training adaptations in older adults using 31P MRS to evaluate skeletal muscle mitochondrial function.Methods
Twenty-eight healthy, sedentary older adults (67±5 yrs old, BMI=30±5, mean±SD, 5 males) participated in a 12-week randomized graded treadmill walking intervention and were assigned to exercise or control groups. Many of these participants were part of a previous study on muscle BOLD increases with exercise training8. Statin use was open label with most patients taking 10 or 20 mg and most commonly using simvastatin. For the exercise group, 6 subjects were on a statin (EX+S) and 8 were not taking a statin (EX). For the control group, 8 were on a statin (CON+S) and 6 were not taking statins (CON). For the exercise groups, walking was done 4 days a week for 45 minutes at 70% heart rate reserve. Controls were asked to maintain a sedentary lifestyle. 31P MRS was used to quantify oxidative capacity of the plantar flexor muscles before and after training. Spectra were acquired using a 12cm surface coil placed under the largest region of the calf (GE Excite 3T MRI, 51.7MHz, TR=3s. 2500Hz sweep, 60° pulse). Subjects performed 30-s of plantar flexion at 0.7 Hz for a total of 20 contractions. MRS data were processed with JMRUI AMARES algorithm. A monoexponential model was used to fit the time constant of phosphocreatine recovery following exercise. Repeated measures ANOVA was used to assess changes in oxidative capacity between groups with significance at p <0.05.Results and Conclusions
A stack plot is shown in Fig. 1 for an individual in the EX+S group before exercise training. PCr changes are shown in Fig. 2 for each group. The acute plantar flexion exercise resulted in ~25% phosphocreatine hydrolysis. Prior to the exercise intervention, PCr time constant (tau,s) was significantly prolonged in statin users (statin use = 42.2±10.5s; no statin use =34.1±9.9s, mean±SD; p=0.039). Following exercise training, the time constant was reduced by 28.0% for EX+S and 25.3% for EX (p<0.001, Fig.3) reflecting an improvement in muscle oxidative capacity. Statin use did not have an independent effect on the adaptation in muscle oxidative capacity. There were no changes in muscle oxidative capacity in the control groups. In conclusion, moderate exercise training in older adults with low dose statin use resulted in typical increases in skeletal muscle mitochondrial function. Improvements in mitochondrial function of thigh muscles have been blunted in past studies of statin treatment and exercise training in middle-aged obese adults at risk for metabolic syndrome6. The successful adaptations of the current intervention may be attributed to low dose statin use with exercise training. It is possible that proximal muscles, like the knee extensors, may respond differently as proximal muscle weakness, soreness and pain have been documented with statin use9. These results are encouraging for the majority of older adults as 50% or more are likely to be prescribed a statin for control of blood cholesterol, reduction in cardiovascular event risk or prevention of metabolic syndrome. 31P MRS can easily be applied across multiple muscle groups, including the knee extensors3, supporting the use of 31P MRS to monitor changes in mitochondrial function in statin users.Acknowledgements
Supported by NIH AG042041.References
- Ridker et al., Lancet, 373:1175-82, 2009.
- Baker SK. Muscle Nerve, 31:572-80, 2005.
- Slade, Forbes et al., Proc Int Mag Reson Med 18:3235, 2010.
- Allard, Schirris et al., J Clin Endocrinol Metab 103(1): 75-84, 2018.
- Dohlmann, Morville et al., J Clin Endo Metab, Epub ahead of print 2018.
- Mikus, Boyle et al., J Am Coll Card 62(8): 709-14, 2013.
- Southern, Nichenko et al., PLoS One, 12(2), 2017.
- Slade, Tonson et al., Proc Int Soc Mag Reson Med 25:87, 2017.
- Dobkin, Neurorehabil Neural Repair;19(3):259-63, 2005.
Figures
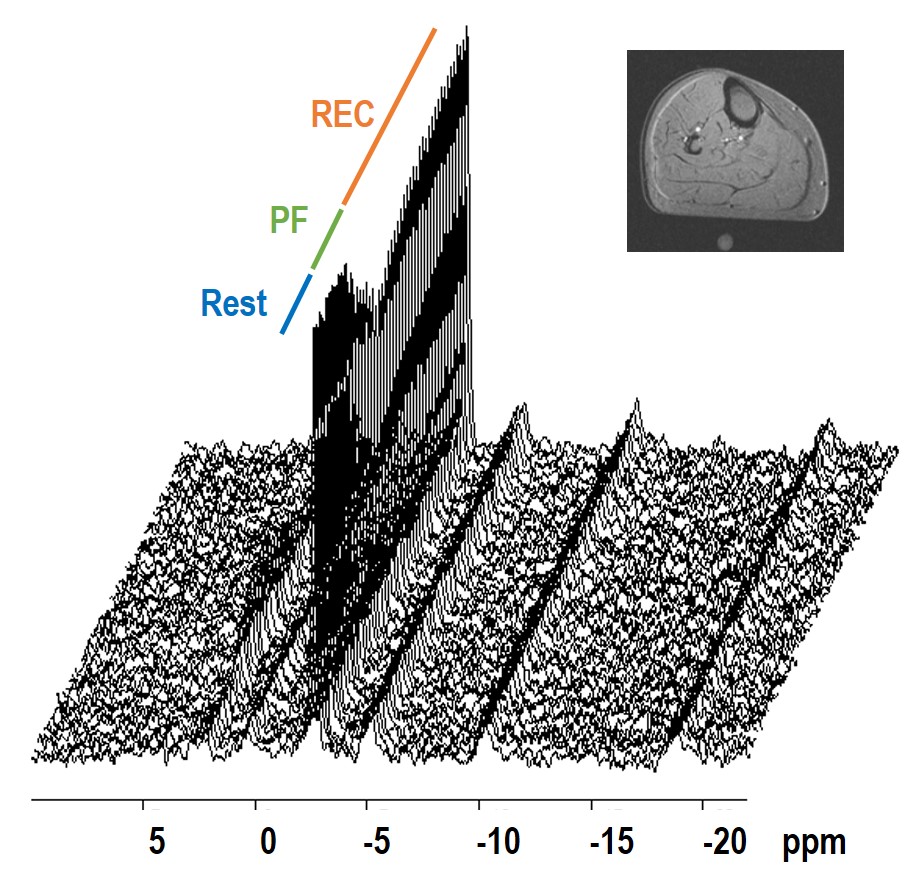
Fig. 1. 31P MRS
stack plot for a representative statin user prior to the exercise intervention. Spectra
are during 30s rest (R), 30s plantar flexion (PF) and 90s recovery (REC). TR=3,
total of 50 spectra shown. The inset image shows the location of the coil with
a tube of water indicating the coil center.
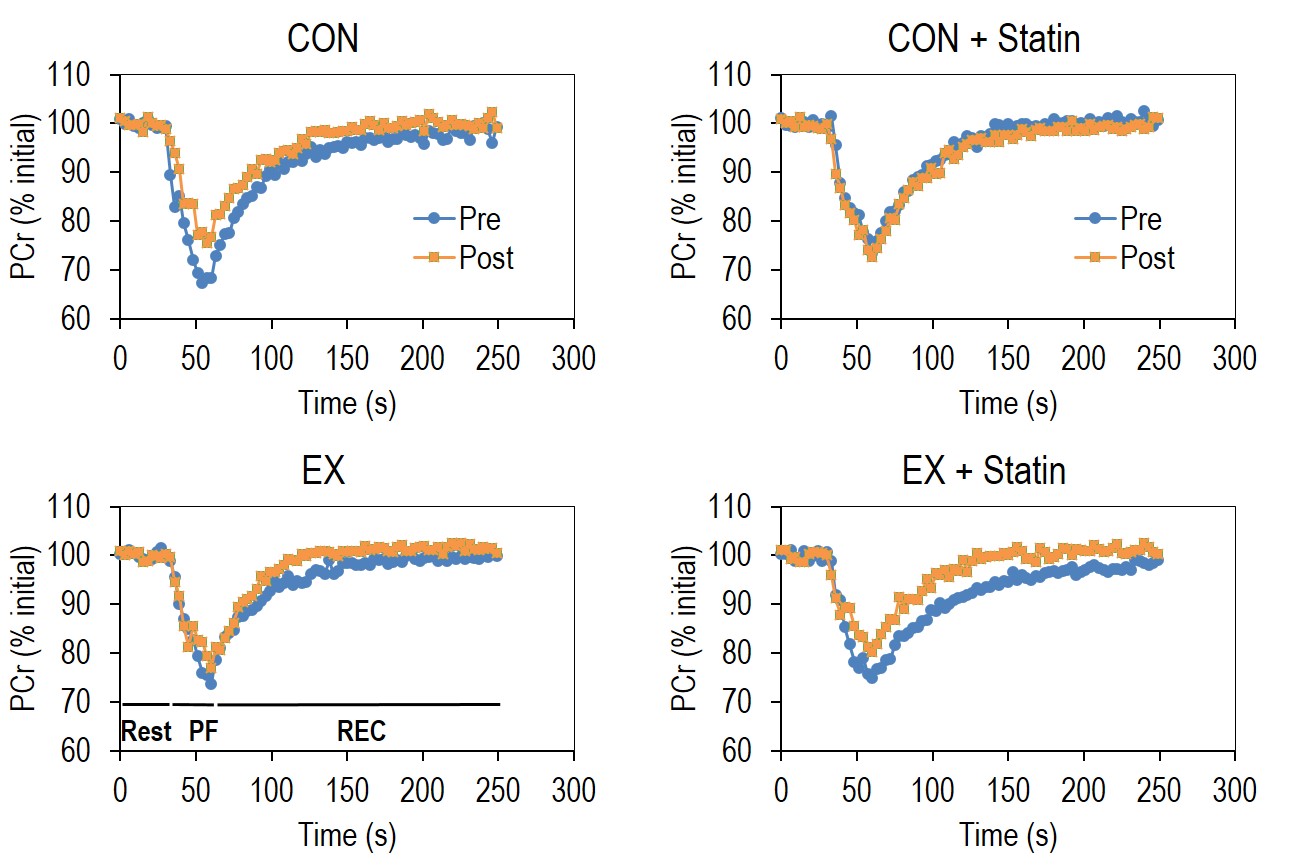
Fig. 2. 31P MRS measured PCr changes during a plantar flexion exercise protocol are plotted for each group before (pre) and after (post) the
intervention period. PCr changes are
shown during 30s rest (R), 30s plantar flexion (PF) and 180s recovery (REC).
Group mean values are plotted.
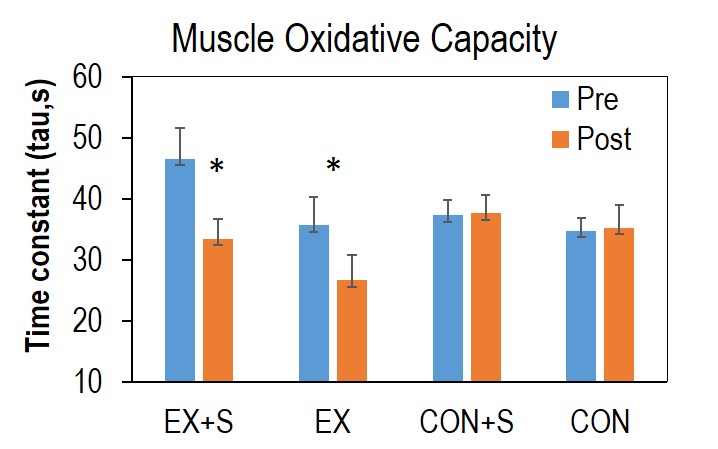
Fig. 3. Group changes in muscle oxidative capacity
following the intervention period. *p<0.05, significant pre-post difference
compared to CON. Data are mean ± SE.