1259
Characterizing respiratory muscle composition and function in Duchenne muscular dystrophy using dynamic MRI and chemical shift-encoded imaging1Department of Physical Therapy, University of Florida, Gainesville, FL, United States, 2Department of Physiology and Functional Genomics, University of Florida, Gainesville, FL, United States
Synopsis
In Duchenne muscular dystrophy (DMD), respiratory muscle weakness leads to eventual respiratory failure. For this investigation, dynamic MRI was utilized to characterize diaphragm and chest wall dynamics during breathing, and chemical shift-encoded imaging was utilized to assess fatty infiltration in accessory respiratory muscles in 36 individuals with DMD and 12 unaffected controls. For maximal inspirations, individuals with DMD had significantly reduced anterior-posterior chest expansion, and a subgroup with poor respiratory function had decreased diaphragm descent (normalized to height). The expiratory muscles had high levels of fatty infiltration, and muscle fat fraction was correlated with measures of expiratory muscle strength.
Introduction
Duchenne muscular dystrophy (DMD) is a progressive muscle degenerative disease characterized by damage, inflammation, and necrosis of muscle fibers with ultimate replacement by fibrofatty connective tissue.1 Dystrophic muscles become weak resulting in impaired mobility, cardiac dysfunction, and respiratory dysfunction, and respiratory impairment is a major cause of morbidity and mortality in DMD. A decrease in expiratory function is often the first sign of respiratory impairment, reflected by a decrease in maximal expiratory pressure (MEP), a measure of expiratory muscle strength.2 This is followed by decreases in both forced vital capacity (FVC), a global measure of pulmonary function, and maximal inspiratory pressure (MIP), a measure of inspiratory muscle strength.2,3 Continued decline leads to eventual respiratory failure. MRI offers a unique method to assess respiratory muscle health and function in vivo in DMD, yet there has been only preliminary work examining diaphragm and chest wall motion using MR methods.4,5 Therefore, the aim of this project was to investigate the pattern of respiratory muscle involvement and chest wall dynamics in DMD using quantitative MR methods.Methods
36 participants with DMD (ages 7-18 years old) and 12 unaffected controls (ages 6-18 years old) underwent an MRI exam of the thorax and abdomen using a 3T Phillips Achieva MRI and 32-channel chest coil. Dynamic MRI (~5-7 frames/sec) was used to obtain sagittal slices through the right lung during free breathing, maximal inspirations, and maximal expirations. Diaphragm and chest wall movement was quantified during breathing. Additionally, chemical shift-encoded (CSE) imaging was performed to examine accessory respiratory muscle fatty infiltration. We acquired coronal chest, axial chest, and axial abdominal images using a single-slice, free breathing protocol with SENSE acceleration for chest images. Parameters were as follows: TR= 10ms (gated), TE= 5.4, 6.4, 7.4ms, flip angle= 3o and 10o, slice thickness= 6mm, resolution= 0.6 X 0.6mm2, NSA=6. Images were reconstructed using a seven peak precalibrated lipid model to produce fat and water images. Fat fraction (FF) was determined for the accessory respiratory muscles of expiration (external oblique, internal oblique, and rectus abdominis) using the formula FF = (fat signal) / (fat+water signal). After MRI acquisition, participants completed clinical tests of pulmonary function including forced vital capacity (FVC), maximal inspiratory pressure (MIP), and maximal expiratory pressure (MEP) measures.Results
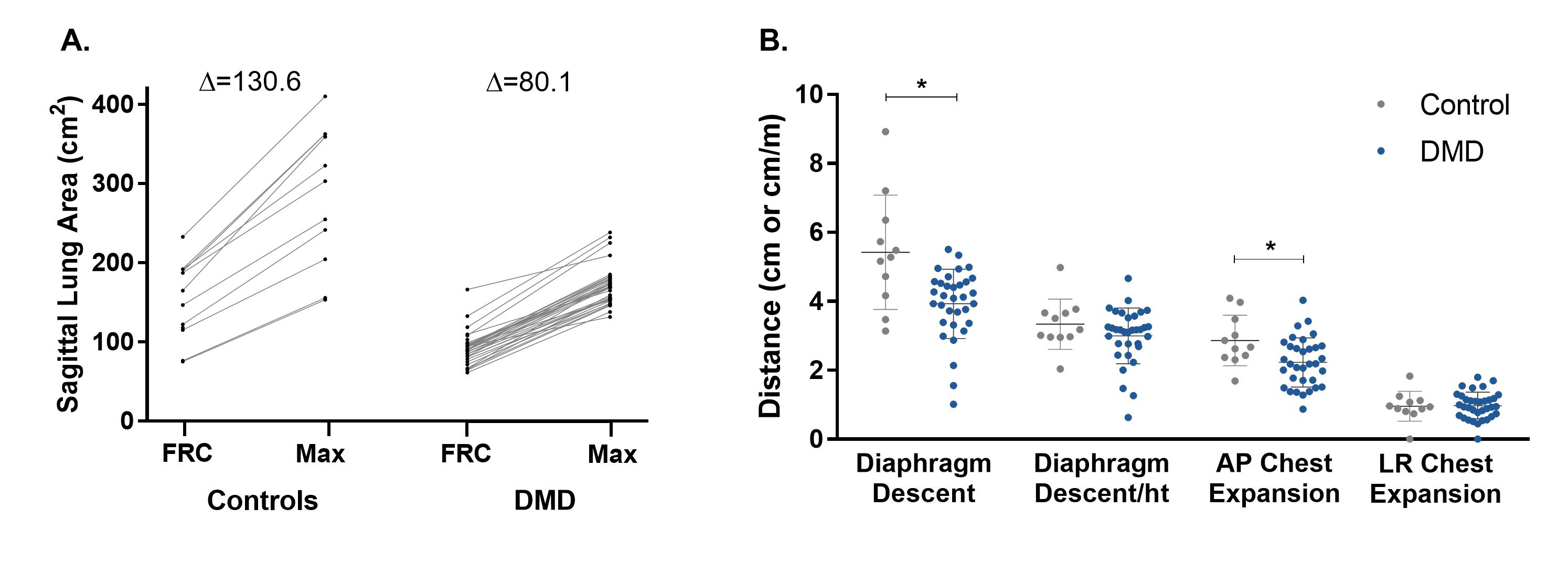
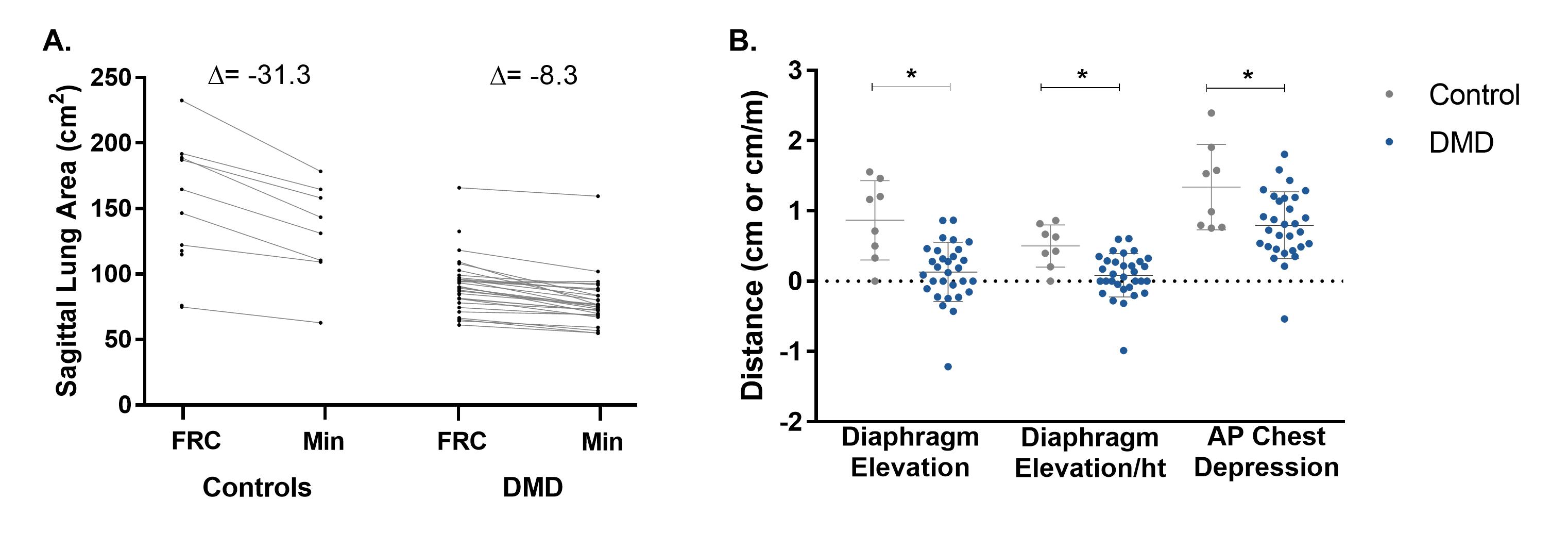
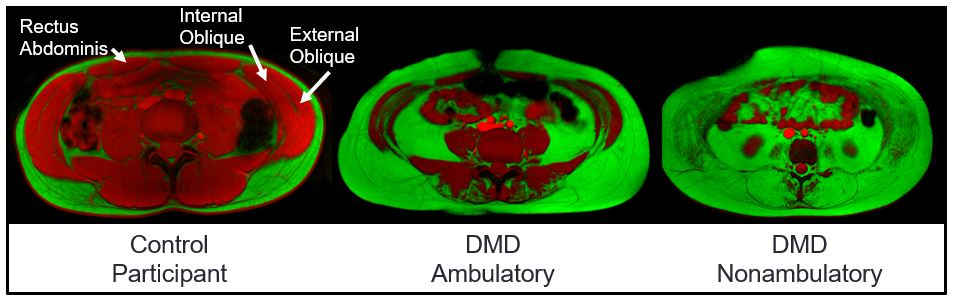
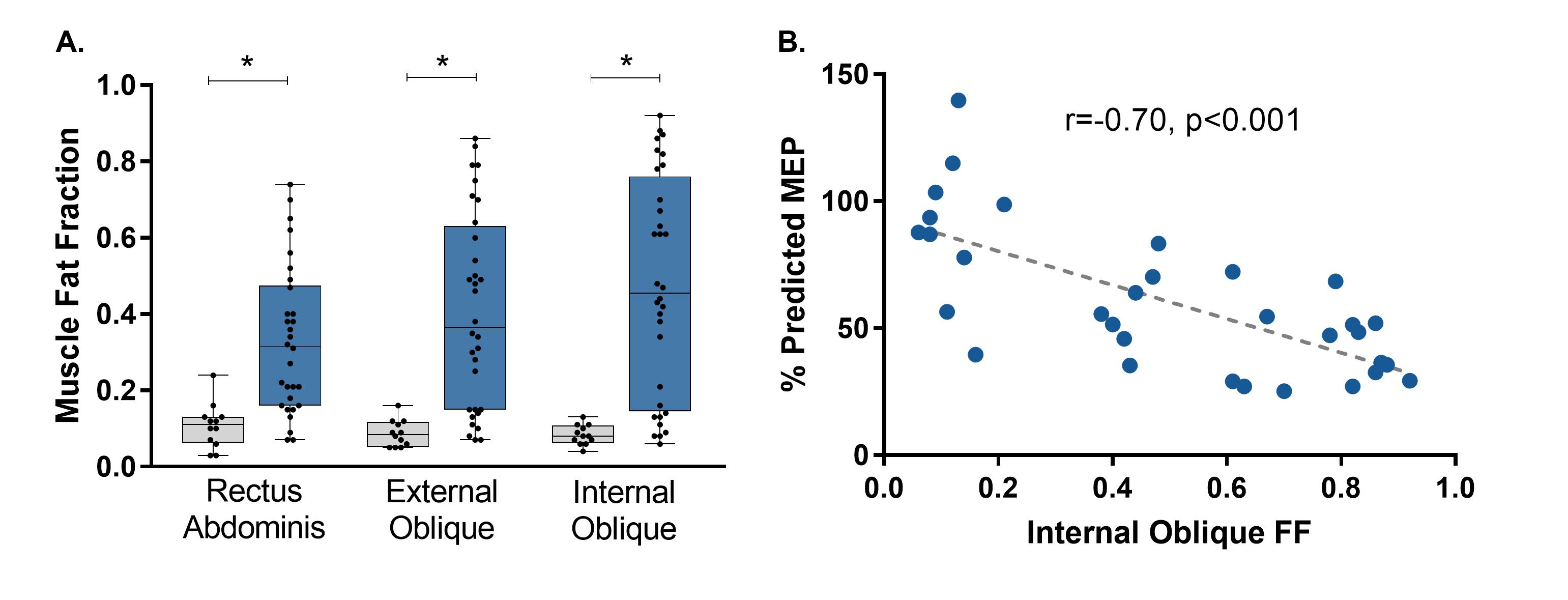
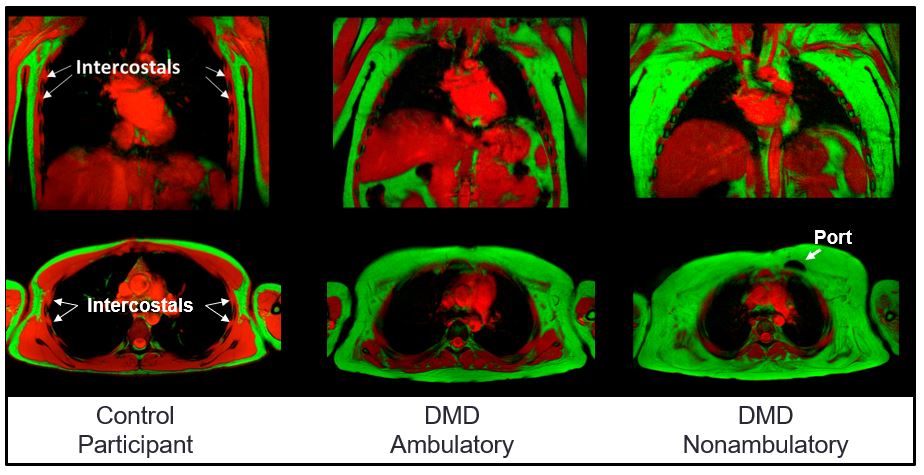
Participants with DMD had impaired FVC, MIP, and MEP values compared to controls (p<0.001 for all tests). Dynamic imaging revealed that individuals with DMD had smaller increases in sagittal plane lung area during maximal inspirations (p=0.003; FIG 1) and smaller decreases in lung area during maximal expirations (p<0.001; FIG 2). Additionally, diaphragm descent was decreased during maximal inspirations, but when descent was normalized to height, only individuals with MIPs≤60% predicted had impaired diaphragm descent (FIG 1B). Chest movement in the anterior-posterior direction was reduced during maximal breathing in DMD compared to controls. CSE MRI revealed significantly elevated expiratory respiratory muscle FF compared to controls with mean FF=0.32 (p<0.001) in the rectus abdominis; FF=0.41 (p<0.001) in the external oblique, and FF=0.49 (p<0.001) in the internal oblique (FIG 3 and FIG 4). MEP was negatively correlated to the FF of the internal oblique muscle (r=-0.70, p<0.001). Visual inspection of the CSE MRI of the chest revealed that the intercostal muscles tended to have minimal fatty infiltration in individuals with DMD, even in individuals with nearly complete fatty replacement of other muscles of the chest (FIG 5).Conclusions
Dynamic MRI and CSE MRI were able to capture novel findings regarding respiratory impairment and respiratory muscle involvement in DMD. Overt MRI signs of diaphragm dysfunction were not present in DMD until inspiratory muscle strength (MIP) was significantly impaired; however, chest mobility during maximal breathing was reduced even in some individuals with normal pulmonary function tests. Failed regeneration of skeletal muscle in DMD leads to significant fatty infiltration of the chest and expiratory muscles yet a relative sparing of the intercostal muscles, and high amounts of fatty infiltration of the expiratory respiratory muscles are reflected functionally as reduced expiratory muscle strength. These findings contribute to a better characterization of respiratory muscle involvement in DMD, and future development of these MR measures as biomarkers may be useful to help determine intervention efficacy.Acknowledgements
Thank you to the participants and their families for their participation in this study, and thank you to the MR technologists for their assistance with data collection. Funding included support from: Failed Regeneration in the Muscular Dystrophies: Inflammation, Fibrosis, and Fat (NIAMS: U54R05264601); Magnetic Resonance Imaging and Biomarkers in Muscular Dystrophy (NIAMS: R01 AR056973); and Interdisciplinary Training in Rehabilitation and Neuromuscular Plasticity (NICHD: T32 HD043730).References
1. Peverelli L, Testolin S, Villa L, et al. Histologic muscular history in steroid-treated and untreated patients with Duchenne dystrophy. Neurology. 2015;85(21):1886–1893.
2. Hahn A, Bach JR, Delaubier A, et al. Clinical implications of maximal respiratory pressure determinations for individuals with Duchenne muscular dystrophy. Arch. Phys. Med. Rehabil. 1997;78(1):1–6.
3. LoMauro A, Romei M, Gandossini S, et al. Evolution of respiratory function in Duchenne muscular dystrophy from childhood to adulthood. Eur. Respir. J. 2018;51(2):1701418.
4. Bishop CA, Ricotti V, Sinclair CDJ, et al. Semi-automated analysis of diaphragmatic motion with dynamic magnetic resonance imaging in healthy controls and non-ambulant subjects with Duchenne muscular dystrophy. Front. Neurol. 2018;9(9).
5. Mankodi A, Kovacs W, Norato G, et al. Respiratory magnetic resonance imaging biomarkers in Duchenne muscular dystrophy. Ann. Clin. Transl. Neurol. 2017;4(9):655–662.
Figures