1251
Multicontrast Distortion-free MRI Using PSF-EPI1Center for Biomedical Imaging Research, Department of Biomedical Engineering, School of Medicine, Tsinghua University, Beijing, China, 2Philips Healthcare, Beijing, China, 3School of Computer Science and Technology, Beijing Institute of Technology, Beijing, China, 4A. A. Martinos Center for Biomedical Imaging, Department of Radiology, Massachusetts General Hospital, Charlestown, MA, United States, 5Harvard-MIT Health Sciences and Technology, MIT, Cambridge, MA, United States, 6Vascular Imaging Laboratory, Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
Fast multimodal exams are required in many situations such as acute ischemic stroke and brain trauma. Recently a multicontrast full brain protocol was proposed based on single shot echo-planar imaging (SS-EPI). However, the SS-EPI images suffer from distortion artifacts. In this work, we provide a speedy multi-contrast distortion-free imaging protocol including T2w, DWI, T2*w, T1 FLAIR and T2 FLAIR based on point spread function encoded echo-planar imaging (PSF-EPI).
Introduction
Fast multimodal exams are required in many situations such as acute ischemic stroke 1-4 and brain trauma 5. Recently a multicontrast full brain protocol was proposed based on single shot echo-planar imaging (SS-EPI) 6. However, the SS-EPI images suffer from distortion artifacts. In this work, we aim to provide a speedy multi-contrast distortion-free imaging protocol including T2w, DWI, T2*w, T1 FLAIR and T2 FLAIR based on point spread function encoded echo-planar imaging (PSF-EPI) 7-9.Materials and Methods
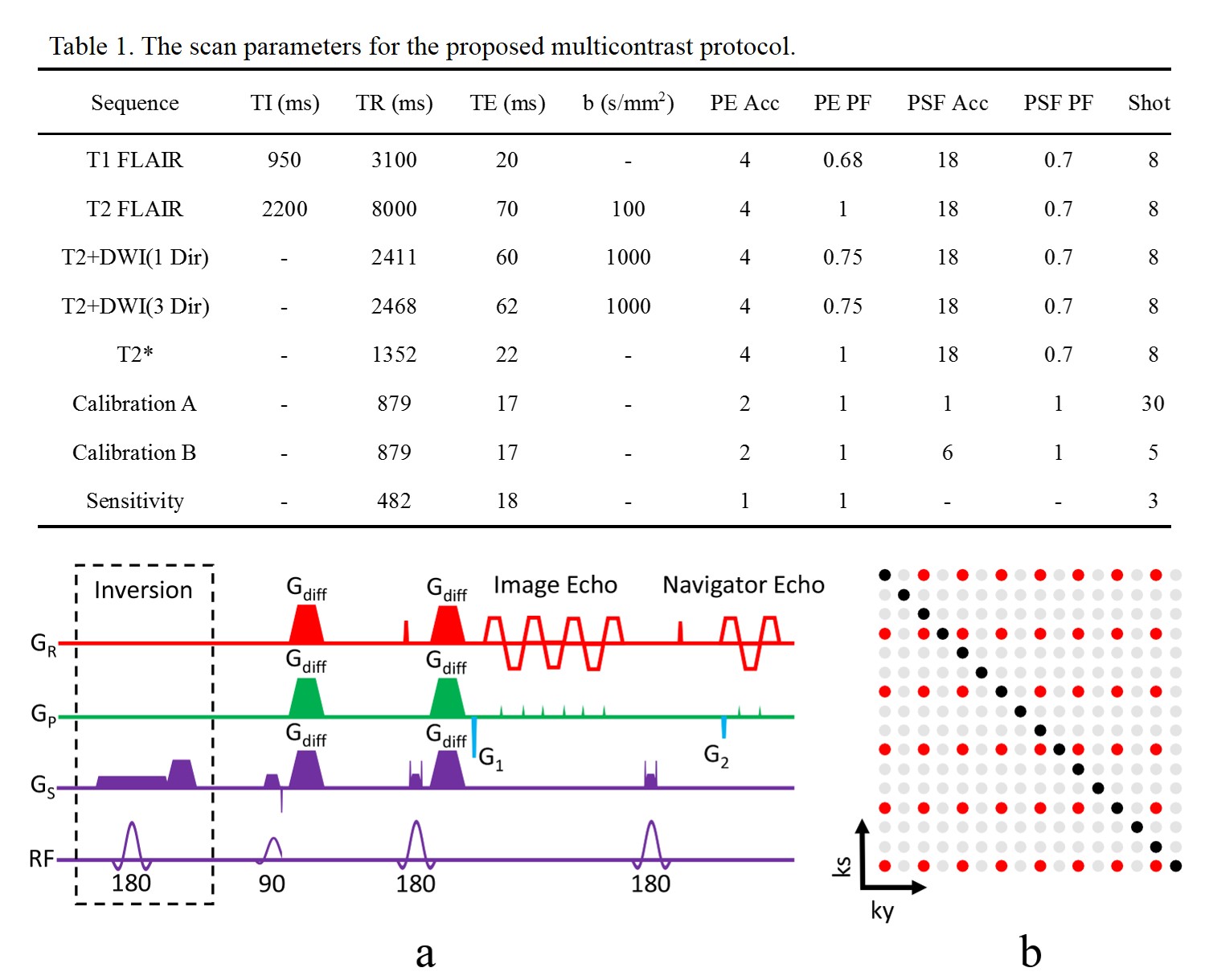
The PSF-EPI sequence was implemented on a Philips 3T Achieva TX scanner (Philips Healthcare, Best, The Netherlands). The sequence diagram is shown in Figure 1. Data were acquired using a 32-channel head coil or an 8-channel head coil. This study was approved by the Institutional Review Board and written informed consent was obtained from all the participants. The acquisition parameters for each contrast are summarized in Table 1. The common scan parameters for the 5 sequences were: field of view (FOV) 220 × 220 mm2, the resolution 1.2 × 1.2 mm2, 24 axial slices with a 4 mm thickness and 1 mm gap were acquired using an anteroposterior phase encoding direction. In order to use Tilted-CAIPI for the reconstruction, two prescans called calibration and sensitivity were acquired to train the GRAPPA kernels 10.
The inversion times (TI) were optimized for the FLAIR sequences on 2 healthy volunteers. A small diffusion weighting (b=0~100 s/mm2) was introduced to suppress inflow artifacts for T2 FLAIR. 3D FLAIR T2 images were acquired as a reference which are almost free of CSF artifacts using a TSE sequence 11-14 with the following parameters: TR/TE/TI = 5000/300/1650 ms with 1.2 mm isotropic resolution, SENSE 1,15 was used for acceleration (AP = 1.4, RL = 2) and the scan time was 3min 45s. 2D T2 TSE images were also acquired as a structural reference with the following parameters: TR/TE = 6200/78 ms, voxel size 1 × 1 × 4 mm3, SENSE was used (AP = 2) and the scan time was 1min 14s. The reconstruction procedure for PSF-EPI was implemented in MATLAB (MathWorks, Natick, MA).
Results
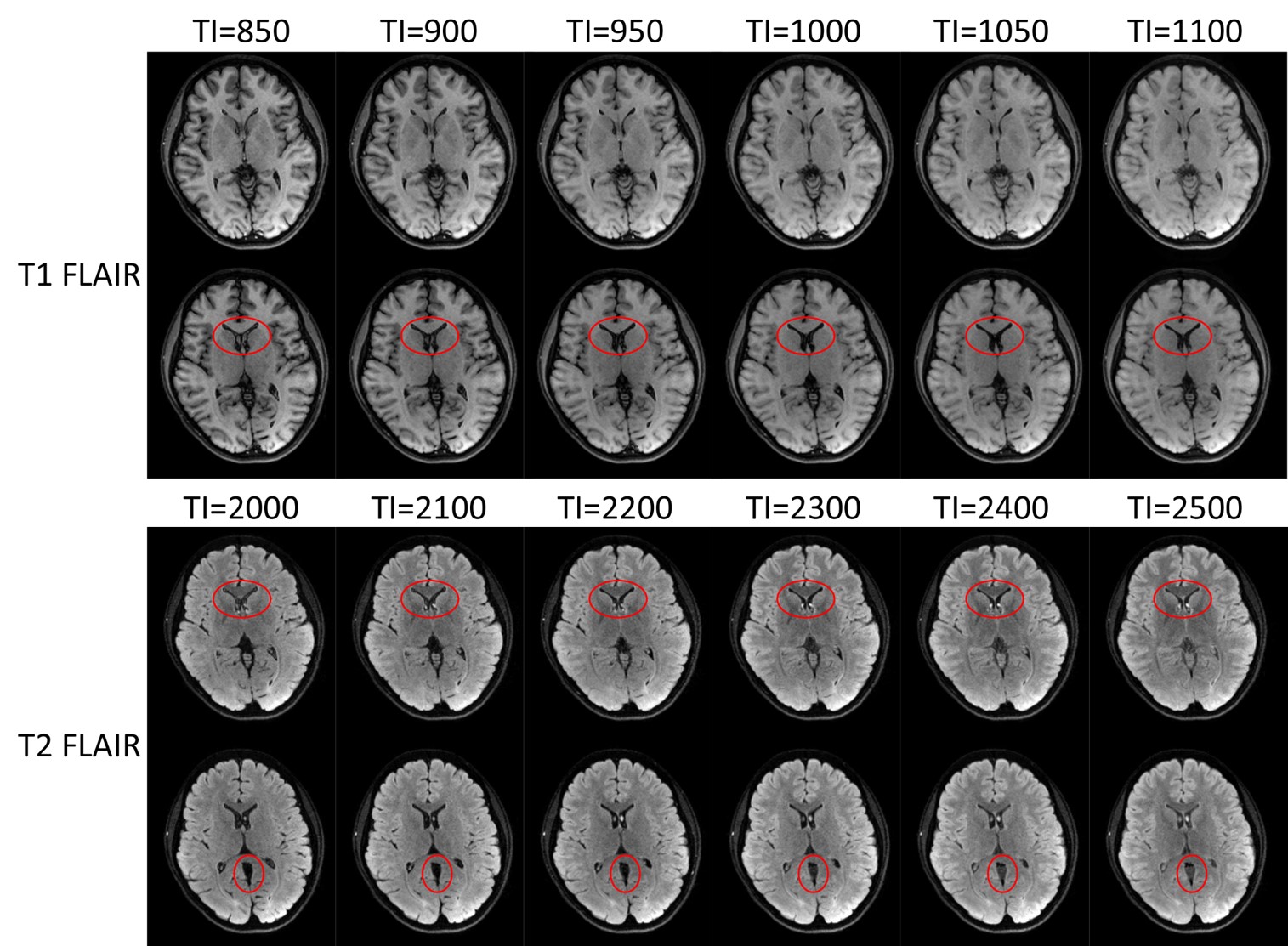
The T1 FLAIR and T2 FLAIR images acquired using variable TIs are shown in Figure 2. For T1 FLAIR, TI = 950 ms achieved optimal suppression of CSF while maintaining sufficient WM / GM contrast. For T2 FLAIR, the optimal suppression of CSF was observed at TI = 2200 ms and the WM/GM contrast was similar for different TIs.
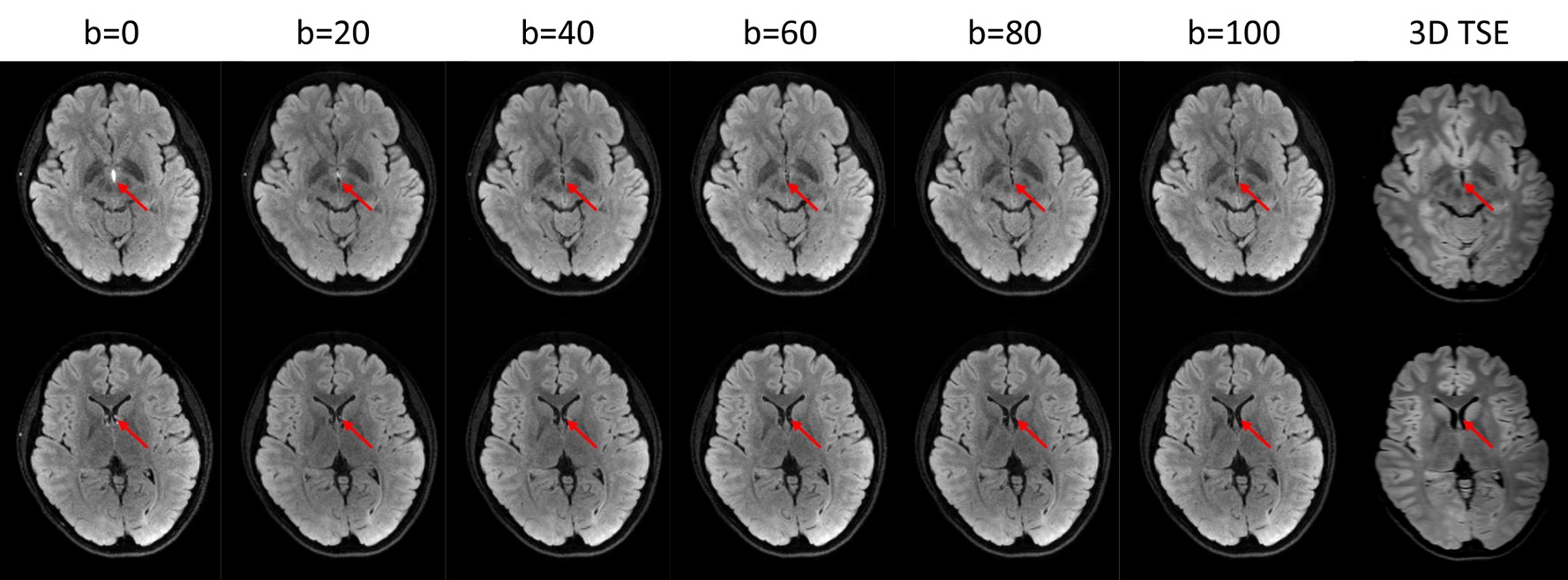
An example of the suppression of inflow artifacts with variable diffusion weighting is shown in Figure 3. Without any diffusion weighting, spurious high intensity signals were observed in the third and the lateral ventricles. With increased diffusion weighting, the high intensity signals were gradually reduced and almost completely suppressed when b=100 s/mm2, as compared to the 3D TSE FLAIR images. It also can be seen that the PSF-EPI FLAIR images have no geometric distortion compared to TSE.
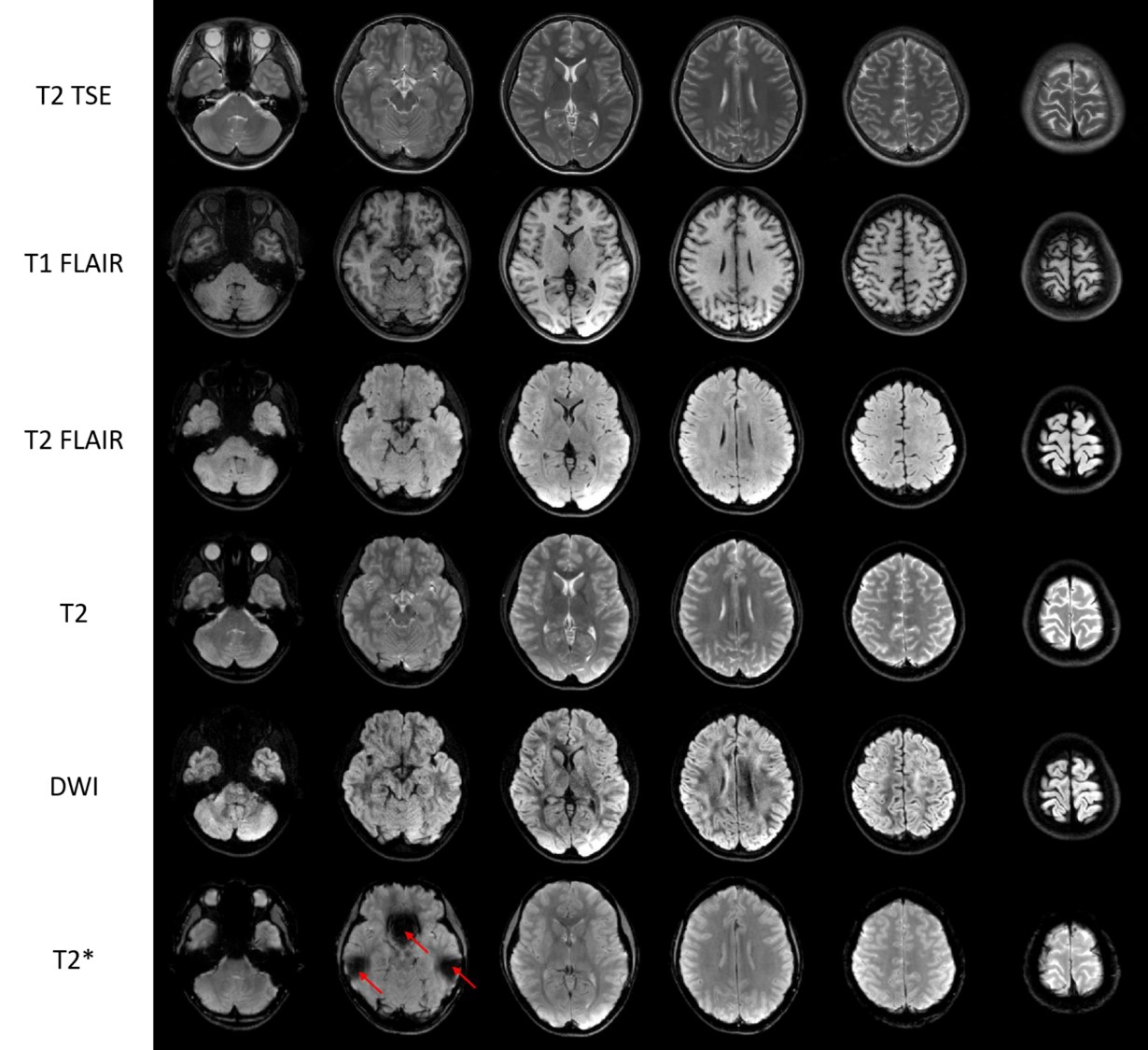
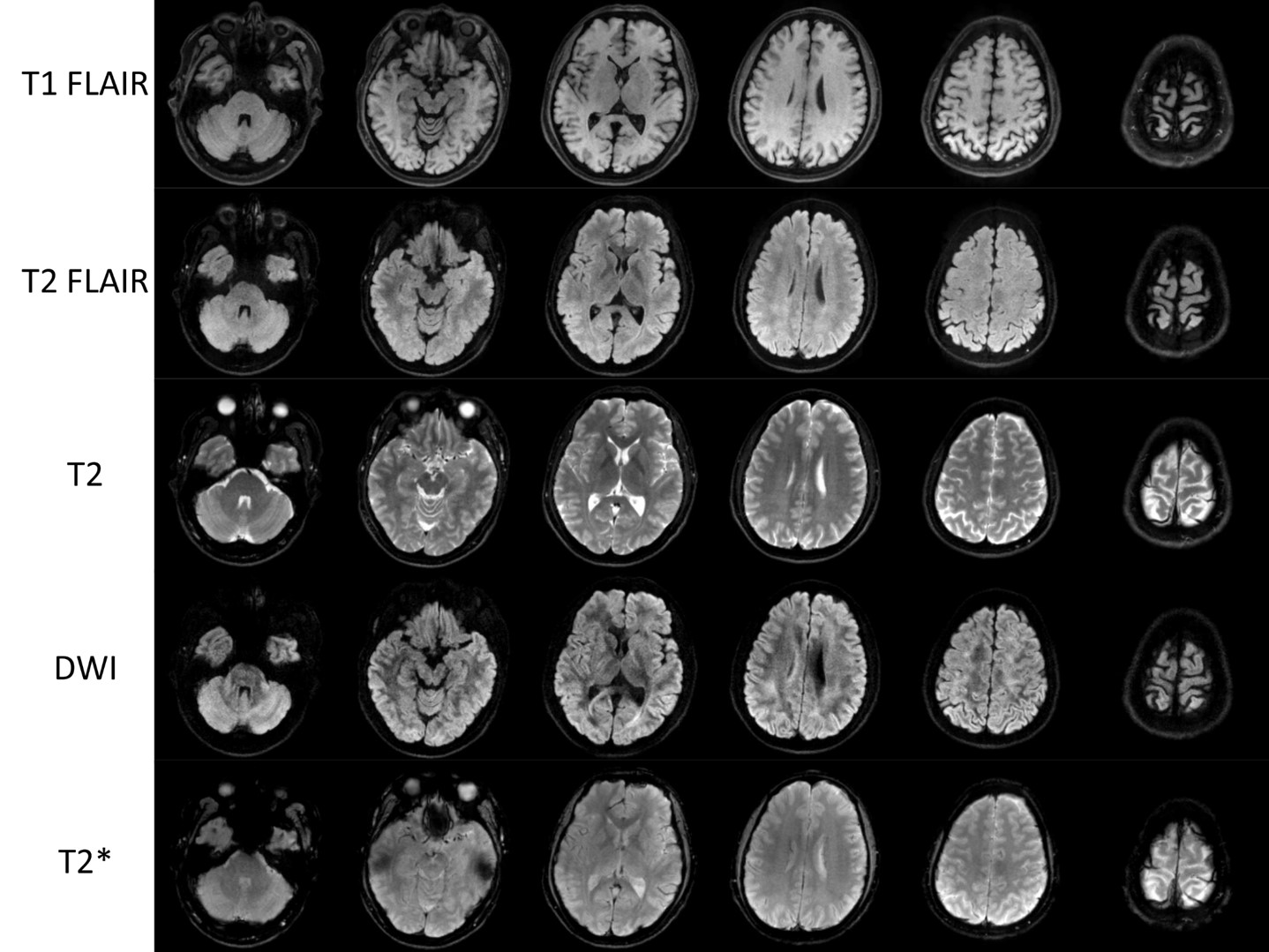
Figure 4 and 5 show exemplary images of all 5 contrasts from 2 subjects acquired using a 32-channel head coil and an 8-channel head coil respectively. The total acquisition time for 5 contrasts (one direction for DWI) and the calibration scans was 232 s. T2 TSE images are also shown in Figure 5 as a reference to demonstrate that the PSF-EPI images were distortion-free. For T2* images, there was signal dropout near the ear canals and the sphenoid. Although the data acquisition was highly undersampled along both PE and PSF directions, the images acquired with an 8-channel head coil shown in Figure 5 have no observable aliasing artifacts.
Discussion and Conclusion
In this study, we proposed a multicontrast distortion-free imaging protocol based on PSF-EPI with Tilted-CAIPI. The protocol features that it inherits the fast acquisition speed of EPI techniques but it is free of geometric distortion and T2* blurring 7,8. The entire acquisition can be carried out with 210 s. The protocol is applicable to head coils with a small number of elements. In general, PSF-EPI provides a basic framework for fast imaging that can also be generalized to more image modalities and tissue quantification. For example, by using intermediate image series 16 and multi-inversion 17, T1, T2 and T2* quantification is possible. A future study should be carried out to compare its clinical significance with conventional multicontrast sequences.Acknowledgements
No acknowledgement found.References
1. Willinek WA, Gieseke J, Falkenhausen Mv, Neuen B, Schild HH, Kuhl CK. Sensitivity Encoding for Fast MR Imaging of the Brain in Patients with Stroke. Radiology 2003;228(3):669-675.
2. Nael K, Khan R, Choudhary G, Meshksar A, Villablanca P, Tay J, Drake K, Coull BM, Kidwell CS. Six-minute magnetic resonance imaging protocol for evaluation of acute ischemic stroke: pushing the boundaries. Stroke 2014;45(7):1985-1991.
3. U-King-Im JM, Trivedi RA, Graves MJ, Harkness K, Eales H, Joubert I, Koo B, Antoun N, Warburton EA, Gillard JH, Baron JC. Utility of an ultrafast magnetic resonance imaging protocol in recent and semi-recent strokes. Journal of Neurology, Neurosurgery & Psychiatry 2005;76(7):1002.
4. Supada P, Thomas W, Susie H, Daniel B, J. BM, Pamela S, Bruce R, Keith H, Eva R, Gilberto G, Otto R. Ultrafast Brain MRI: Clinical Deployment and Comparison to Conventional Brain MRI at 3T. Journal of Neuroimaging 2016;26(5):503-510.
5. Bruno DM. Brain trauma protocol (MRI). Radiopaedia, 2005. Volume 2018.
6. Skare S, Sprenger T, Norbeck O, Rydén H, Blomberg L, Avventi E, Engström M. A 1-minute full brain MR exam using a multicontrast EPI sequence. Magnetic resonance in medicine 2017;00:1-10.
7. Dong Z, Wang F, Reese T, Manhard M, Bilgic B, Wald L, Guo H, Setsompop K. Fast Distortion-Free Diffusion Imaging using “tilted-CAIPI” PSF-EPI. Paris, 2018.p.1204. p 1204.
8. In MH, Posnansky O, Speck O. High-resolution distortion-free diffusion imaging using hybrid spin-warp and echo-planar PSF-encoding approach. NeuroImage 2017;148(June 2016):20-30.
9. Robson MD, Gore JC, Constable RT. Measurement of the point spread function in MRI using constant time imaging. Magnetic resonance in medicine 1997;38(12):733-740.
10. Dong Z, Wang F, Reese TG, Manhard MK, Bilgic B, Wald LL, Guo H, Setsompop K. Tilted-CAIPI for highly accelerated distortion-free EPI with point spread function (PSF) encoding. Magnetic resonance in medicine;0(0).
11. Lummel N, Schoepf V, Burke M, Brueckmann H, Linn J. 3D Fluid-Attenuated Inversion Recovery Imaging: Reduced CSF Artifacts and Enhanced Sensitivity and Specificity for Subarachnoid Hemorrhage. American Journal of Neuroradiology 2011;32(11):2054.
12. Naganawa S, Koshikawa T, Nakamura T, Kawai H, Fukatsu H, Ishigaki T, Komada T, Maruyama K, Takizawa O. Comparison of flow artifacts between 2D-FLAIR and 3D-FLAIR sequences at 3 T. Eur Radiol 2004;14(10):1901-1908.
13. Kallmes DF, Hui FK, Mugler JP, 3rd. Suppression of cerebrospinal fluid and blood flow artifacts in FLAIR MR imaging with a single-slab three-dimensional pulse sequence: initial experience. Radiology 2001;221(1):251-255.
14. Chagla GH, Busse RF, Sydnor R, Rowley HA, Turski PA. Three-dimensional fluid attenuated inversion recovery imaging with isotropic resolution and nonselective adiabatic inversion provides improved three-dimensional visualization and cerebrospinal fluid suppression compared to two-dimensional flair at 3 tesla. Investigative radiology 2008;43(8):547-551.
15. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magnetic resonance in medicine 1999;42(5):952-962.
16. Fuyixue Wang, Zijing Dong, Timothy G. Reese, Berkin Bilgic, Mary Kate Manhard, Lawrence L. Wald, Setsompop K. Echo Planar Time-resolved Imaging (EPTI). 2018; Paris. p 0217.
17. Cohen O, Polimeni JR. Optimized inversion-time schedules for quantitative T1 measurements based on high-resolution multi-inversion EPI. Magnetic resonance in medicine 2018;79(4):2101-2112.
Figures