1241
A 12-channel flexible receive coil for accelerated tongue imaging1Department of Head and Neck Surery and Oncology, Netherlands Cancer Institute/Antoni van Leeuwenhoek Hospital, Amsterdam, Netherlands, 2Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands, 3Department of Oral and Maxillofacial Surgery, Academic Centre for Dentistry Amsterdam and Academic Medical Center, Amsterdam, Netherlands, 4MR Coils BV, Zaltbommel, Netherlands, 5Department of Oral and Maxillofacial Surgery, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands, 6Department of Robotics and Mechatronics, MIRA Institute, University of Twente, Enschede, Netherlands, 7Biomedical Engineering and Physics, Amsterdam UMC, University of Amsterdam, Amsterdam, Netherlands
Synopsis
Acceleration techniques necessary for real-time MRI of swallowing and diffusion imaging of the tongue require multiple coil elements and decrease SNR. Therefore, we designed a 12-channel flexible tongue coil with a higher density of elements compared to the conventional head and neck coil. The SNR in the tongue coil is better, while the G-factor is lower compared to the conventional coil. Real-time MRI displayed better image quality with fewer radial streaking artefacts using the tongue coil. A multiband-SENSE factor of 2 was feasible for diffusion-weighted imaging with the tongue coil.
Purpose
MRI of the tongue often suffers from motion artefacts caused by breathing of swallowing. Motion artefacts can be reduced by shortening the scan time. Acceleration techniques such as compressed sensing are even able to measure multiple motion states of swallowing1. However, application of acceleration techniques will come with reduced SNR and/or image quality. The use of a dedicated multichannel surface coil may alleviate this problem. In this work, we have developed a flexible receive coil containing relatively small coil elements, allowing for the use of compressed sensing (CS) and multiband acceleration (MB) techniques.Methods
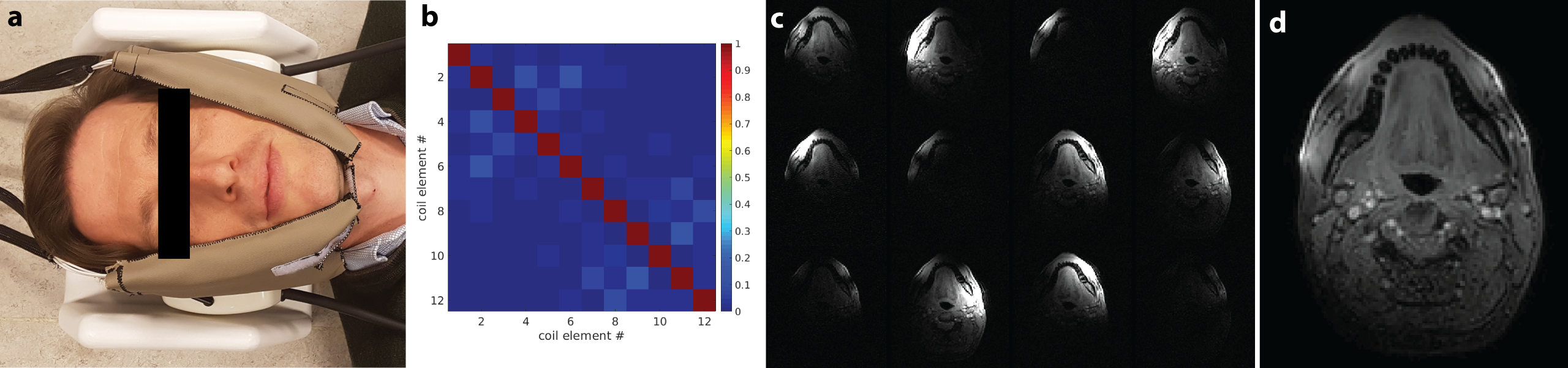
A 12-channel flexible receive coil was designed in collaboration with MR Coils BV (Zaltbommel, Netherlands). Twelve copper coil elements of 53 by 32 mm were assembled in two grids of 2-by-3 elements. The coil elements were tuned and matched while loading the coil with a volunteer (figure 1A).
Three healthy volunteers were included (one female, range 23-28) and written informed consent was collected. The study was approved by the institutional Medical Ethics Review Board. The volunteers were scanned with a 3T Philips Ingenia scanner (Philips Healthcare, Best, Netherlands) using a conventional neurovascular coil first and with the new flexible coil second, and otherwise identical scanning protocol.
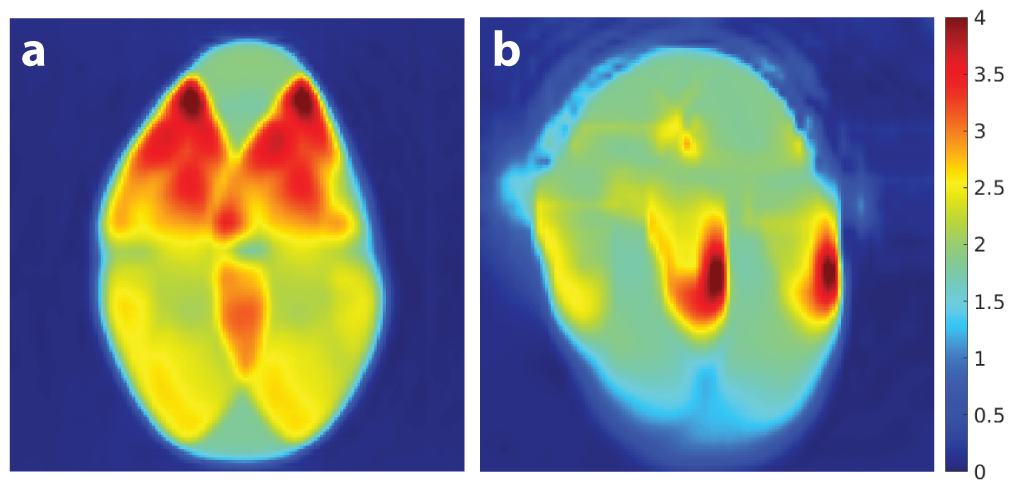
Individual coil element images and SNR maps were created using a 2D FFE sequence with the following parameters: TR/TE: 6.3/3.2 ms; voxel size: 1.25 x 1.25 x 1.25 mm3; flip angle: 8°; no parallel imaging; scan time: 52 s. This sequence was repeated with RF switched off to obtain noise images. G-factor maps were acquired by repeating the previous sequence with SENSE acceleration R = 4.
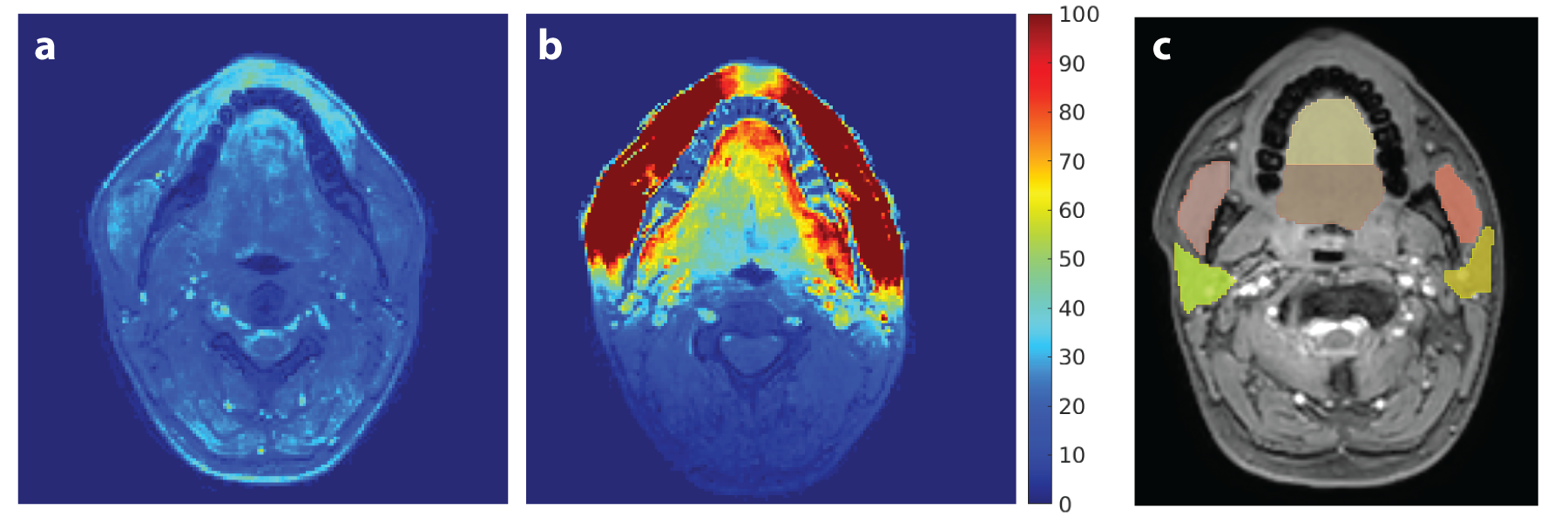
The noise correlation matrix was created by calculating the correlation coefficient of noise images between all possible combinations of coil channels. SNR maps were estimated by dividing the signal by the standard deviation of noise within a radius of five voxels, corrected for the Rician distribution of the noise. The masseter muscle, anterior and posterior tongue, and parotid glands were manually delineated. SNR gain of the flexible coil compared to the conventional coil was calculated for these structures.
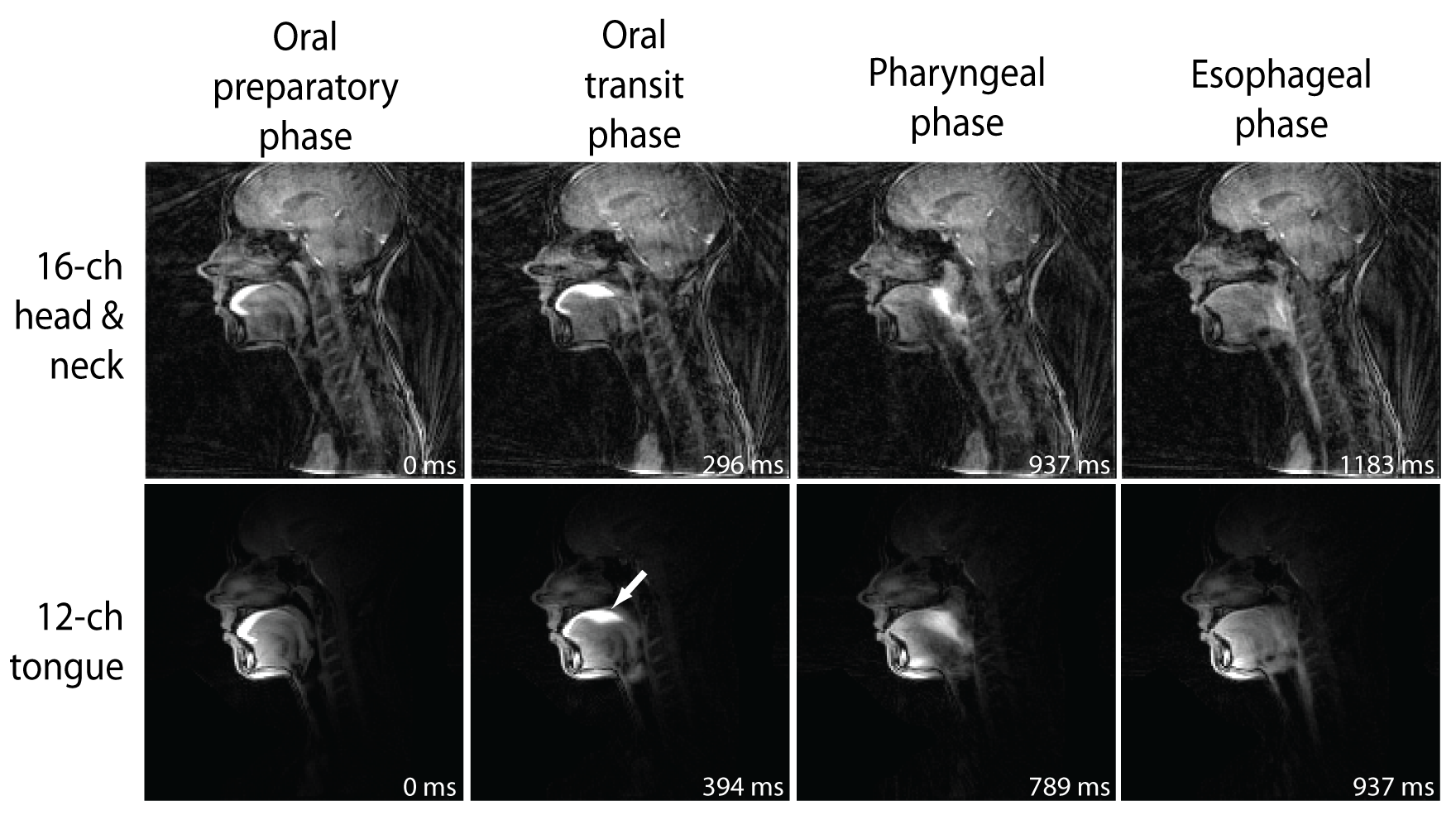
Real-time MRIs during swallowing were acquired using a sagittal single-slice golden angle radial spoiled GRE sequence2, with TR/TE: 2.9/1.12 ms; flip angle: 10°; TFE factor: 22; matrix size: 128 x 128; voxel size: 2 x 2 x 6 mm3; golden angle: 111.25°; dynamic scan time: 10 s. Image reconstruction was performed off-line using BART3. Sensitivity maps were determined using the eSPIRIT-method from low-resolution images containing all spokes4. 34 new spokes were included in each temporal bin, and a sliding window approach was used to double the number of temporal bins, resulting in a frame rate of 20 fps and R = 7.5. Compressed sensing reconstructions were performed using locally low-rank5 and total variation over time constraints with regularisation parameters λ=0.005 and λ=0.05, respectively. Volunteers were asked to swallow pineapple juice, which contains manganese providing T1 contrast.
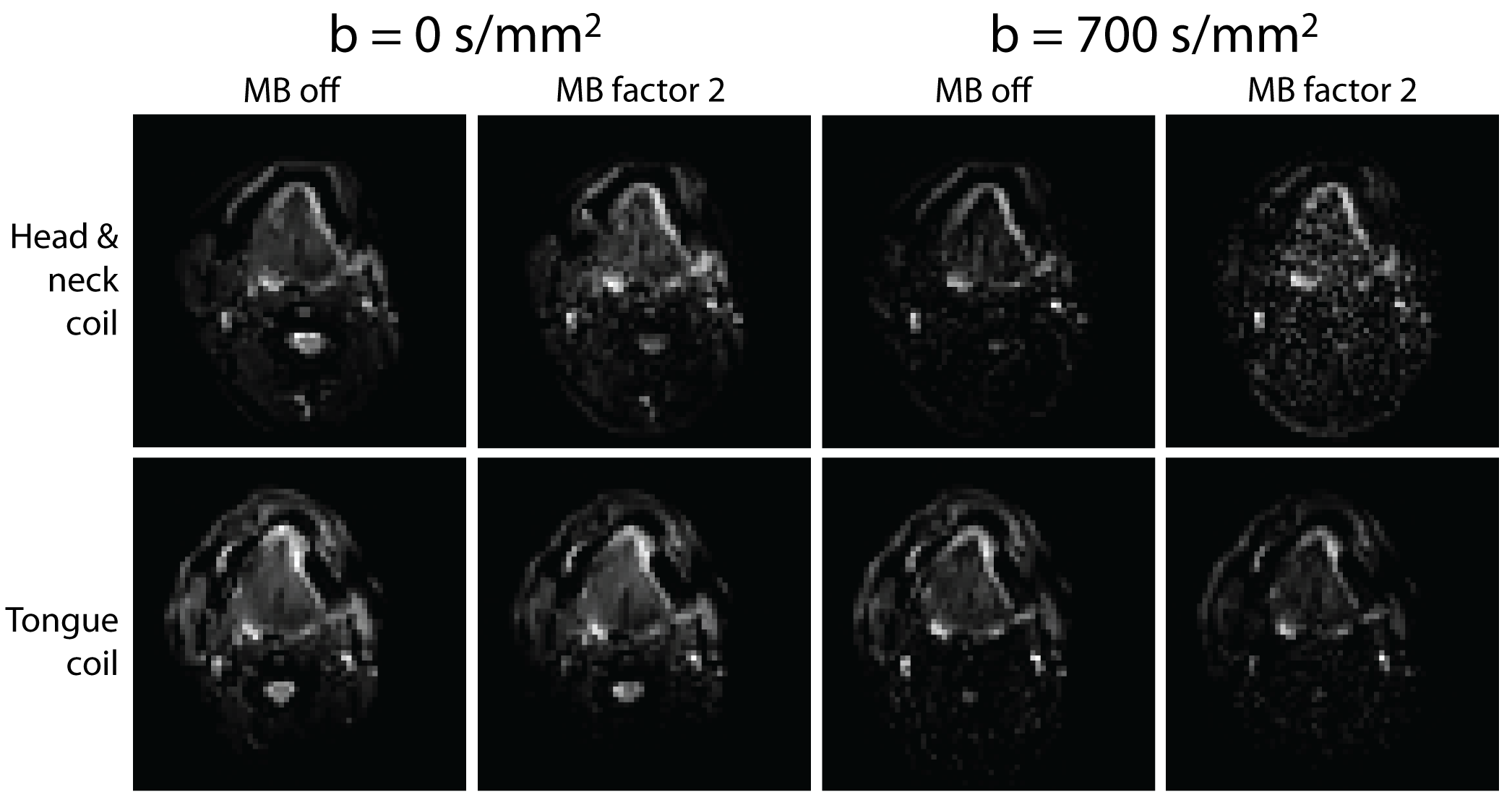
Diffusion-weighted imaging of the tongue was performed using a SE-EPI sequence with TR/TE: 2746/71 ms; ETL: 35; matrix size: 64 x 52; voxel size: 3 x 3 x 3 mm3; within slice SENSE factor: 1.5 along LR direction; no partial Fourier; NSA: 1; SPIR and SSGR fat suppression; b-value: 700 s/mm2 along 6 directions; total scan time: 24.7 s. The whole acquisition was repeated using MB-SENSE factor 2 (scan time: 12.6 s).
Results
Figure 1B shows that there is low correlation between coil elements and thus minor coupling. Signals from individual coil elements are highly localized around the coil elements (figure 1C), but provide sufficient overlap to cover the full jaw and tongue anatomy (figure 1D) and to allow for efficient SENSE acceleration. This is evident from the G-factor maps, in which the flexible coil performs better with lower and more homogeneously distributed G-factor (figure 2). The new coil provides superior SNR (figure 3A,B) in the cheeks close to the coil elements, but importantly also in the tongue. Real-time MRI of swallowing is feasible with the flexible tongue coil, without the streaking artefacts and noise present in the images for the conventional coil (figure 4). MB-SENSE acceleration of diffusions-weighted images (figure 5) displays noise enhancement for the conventional coil, while this was not observed with the flexible coil.Discussion
The 12-channel flexible coil design has better SNR in the tongue and lower G-factor allowing higher acceleration factors. Imaging techniques such as real-time MRI of swallowing and MB-SENSE for diffusion imaging of the tongue perform better with the flexible coil than with the conventional coil.Acknowledgements
We would like to thank the Maurits en Anna de Kock Stichting for kindly providing a grant for the purchase of the 12-channel flexible coil.References
- Zhang S, Olthoff A, Frahm J. Real-time magnetic resonance imaging of normal swallowing. J Magn Reson Imaging. 2012;35(6):1372-1379. doi:10.1002/jmri.23591.
- Feng L, Grimm R, Block KT obia., et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med. 2014;72(3):707-717. doi:10.1002/mrm.24980.
- Uecker M, Ong F, Tamir JI, et al. Berkeley Advanced Reconstruction Toolbox. In: Proc. Intl. Soc. Mag. Reson. Med. Toronto; 2015. doi:10.5281/zenodo.592960.
- Uecker M, Lai P, Murphy MJ, et al. ESPIRiT - An eigenvalue approach to autocalibrating parallel MRI: Where SENSE meets GRAPPA. Magn Reson Med. 2014;71(3):990-1001. doi:10.1002/mrm.24751.
- Ong F, Lustig M. Beyond low rank+ sparse: Multi-scale low rank matrix decomposition. 2016 IEEE Int Conf Acoust Speech Signal Process. 2016;10(4):4663-4667. doi:10.1109/ICASSP.2016.7472561.
Figures