1240
Brain and head-and-neck MRI in immobilization masks: a novel and practical setup for radiotherapy1University Medical Center Utrecht, Utrecht, Netherlands, 2Utrecht University, Utrecht, Netherlands, 3University of Turin, Turin, Italy
Synopsis
For radiotherapy treatment planning, it is essential to perform the MRI/CT exams in treatment position. For this purpose, thermoplastic immobilization masks are used for brain and head-and-neck radiotherapy. However, since standard immobilization masks do not fit in the diagnostic MR head/neck coils, suboptimal surface-loop coils leading to poor image quality are used in clinical practice. Here, we present a new immobilization setup. This setup has several advantages compared to state-of-the-art setups: it fits in the diagnostic head/neck MR coils, it allows diagnostic image quality in treatment position, high SNR, homogenous signal, restricted motion (about 1 mm) and accurate inter-fraction repositioning.
Introduction
In Radiotherapy (RT) clinical practice, the superior soft tissue contrast of MRI images compared to CT makes MRI an essential image modality. MRI provides multi-contrast visualization of tumors, which allows tumor delineation and monitoring of RT treatments. For RT treatment planning, it is essential to perform the MRI and CT exams in treatment position. For this purpose and to minimize inter/intra-fraction movement, thermoplastic immobilization masks are used for brain and head-and-neck (HN) RT. However, standard immobilization masks do not fit in the diagnostic MR head/neck coils. As a compromise, flexible surface coils are adopted1-6 despite their technician dependent positioning and inferior signal-to-noise-ratio (SNR)7 compared to diagnostic head/neck coils. This leads to relatively poor image quality and reproducibility. The goal of this work is to create a new immobilization setup that fits into the diagnostic MR head/neck coils thereby boosting MR image quality and reproducibility compared to standard RT setups.Materials and Methods
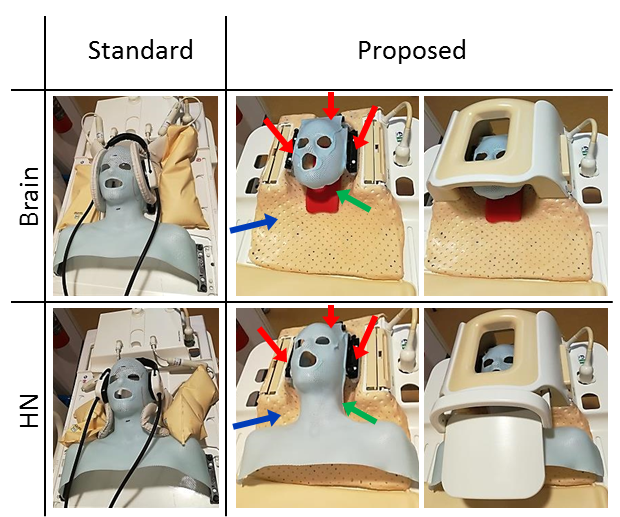
For the standard and the novel RT brain/HN setups (Fig. 1), MR images were acquired on 2 volunteers using a 3T Ingenia MRI (Philips Healthcare, Best, The Netherlands).
The standard RT setup consisted of an individualized five-points head-and-shoulder mask fixated to the MRI flat table top, a standard neck support, and two MR flexible surface receive coils (diameters = 15 cm for HN, 20 cm for brain).
The novel RT setup consisted of an individualized three-points mask (for brain) or three-points head-and-shoulder mask (for neck) that fit into the diagnostic MR head/neck coils. A new fixation thermoplastic base hosting the anchor points for the immobilization masks was created to fit in the MR head/neck base. The proposed setup can be used for both 1.5T and 3T scanners given the same base geometry.
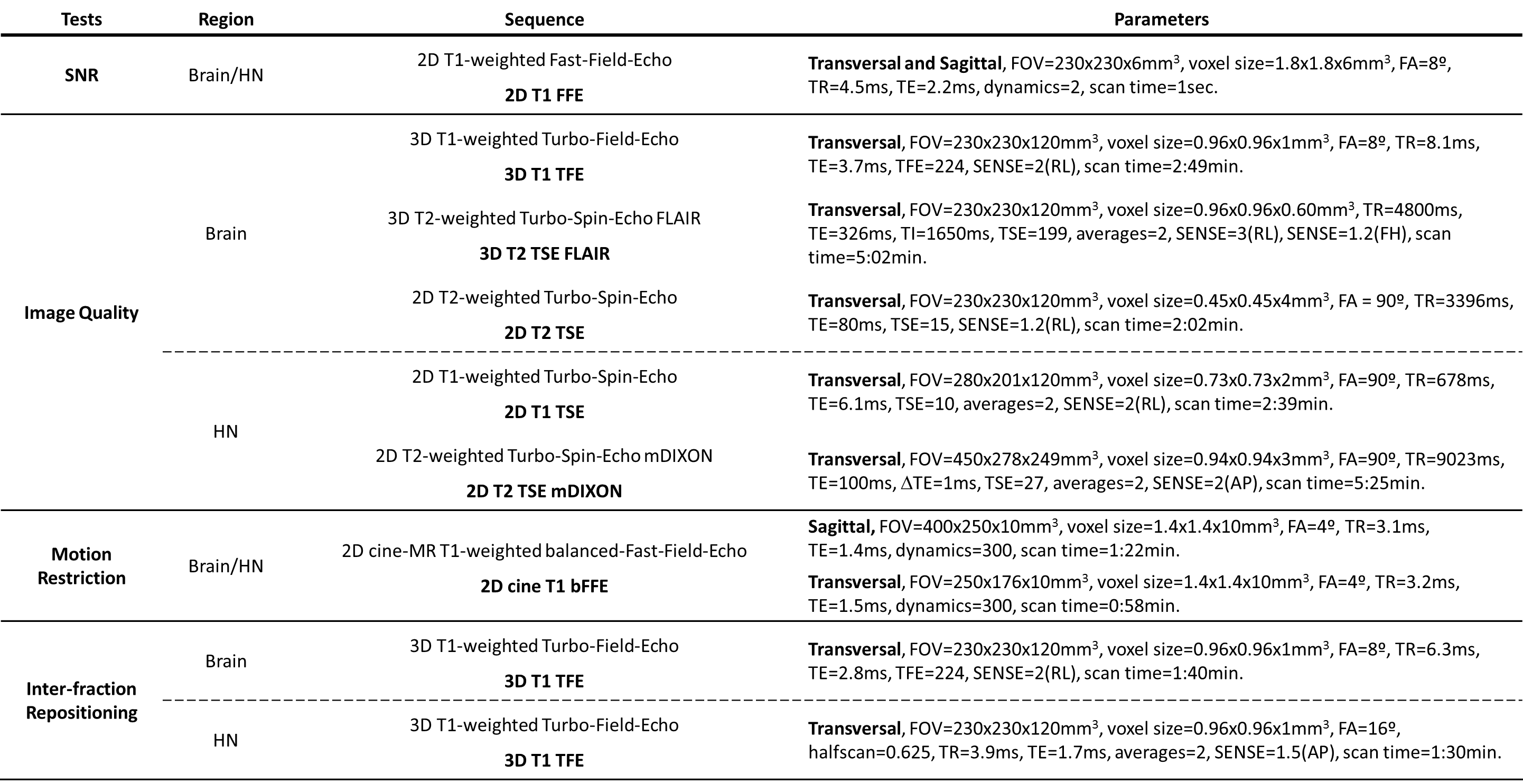
Several comparative tests were performed (Table 1).
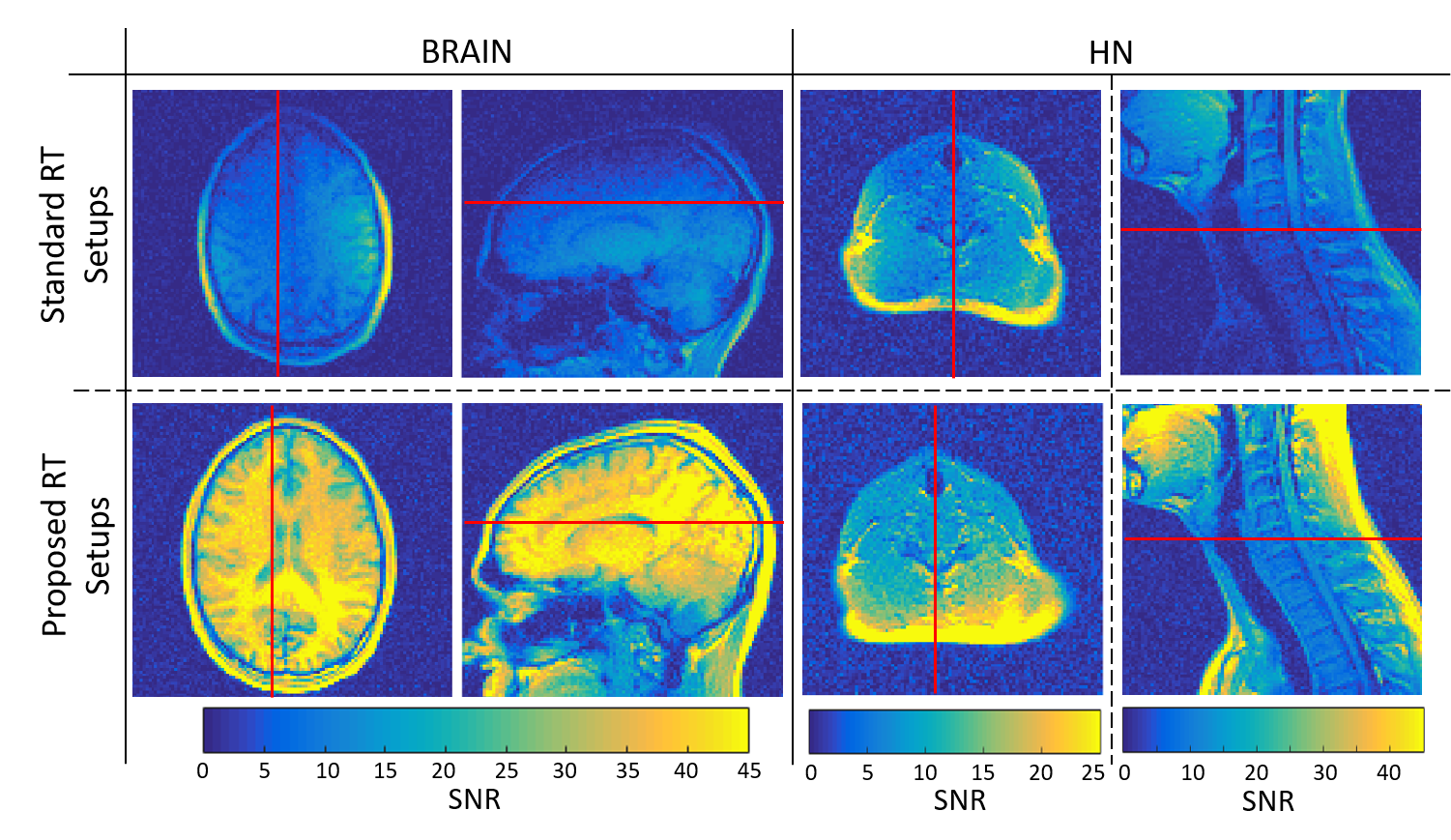
- SNR test: relative SNR maps were computed from 2D T1-weighted Fast-Field-Echo scans (2 dynamics, the second being a noise scan)8.
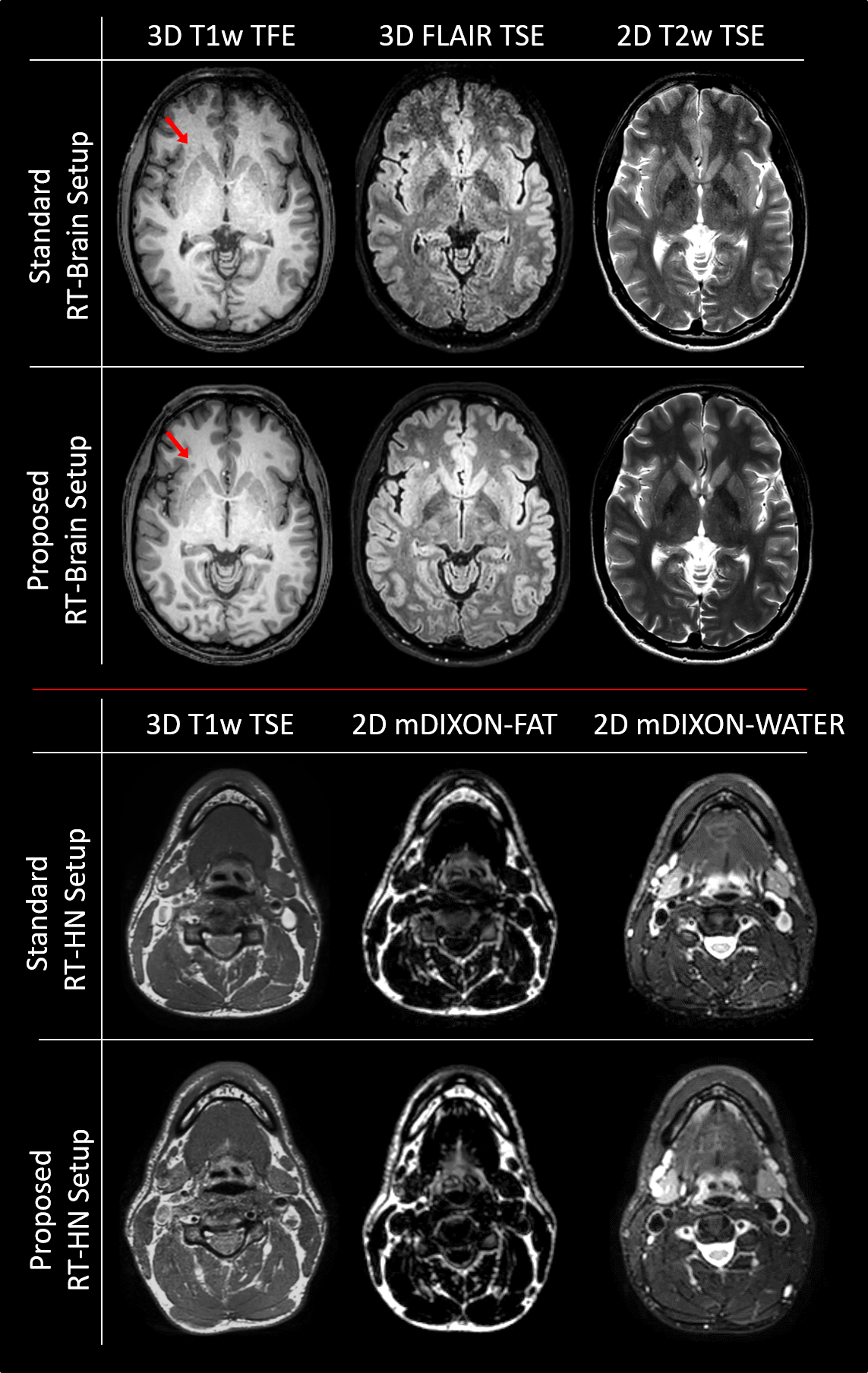
- Image quality test: 3D T1-weighted Turbo-Field-Echo, 3D T2-weighted Turbo-Spin-Echo FLAIR and 2D T2-weighted Turbo-Spin-Echo scans were acquired for brain, for neck 2D T1-weighted Turbo-Spin-Echo and 2D T2-weighted Turbo-Spin-Echo mDIXON scans were acquired.
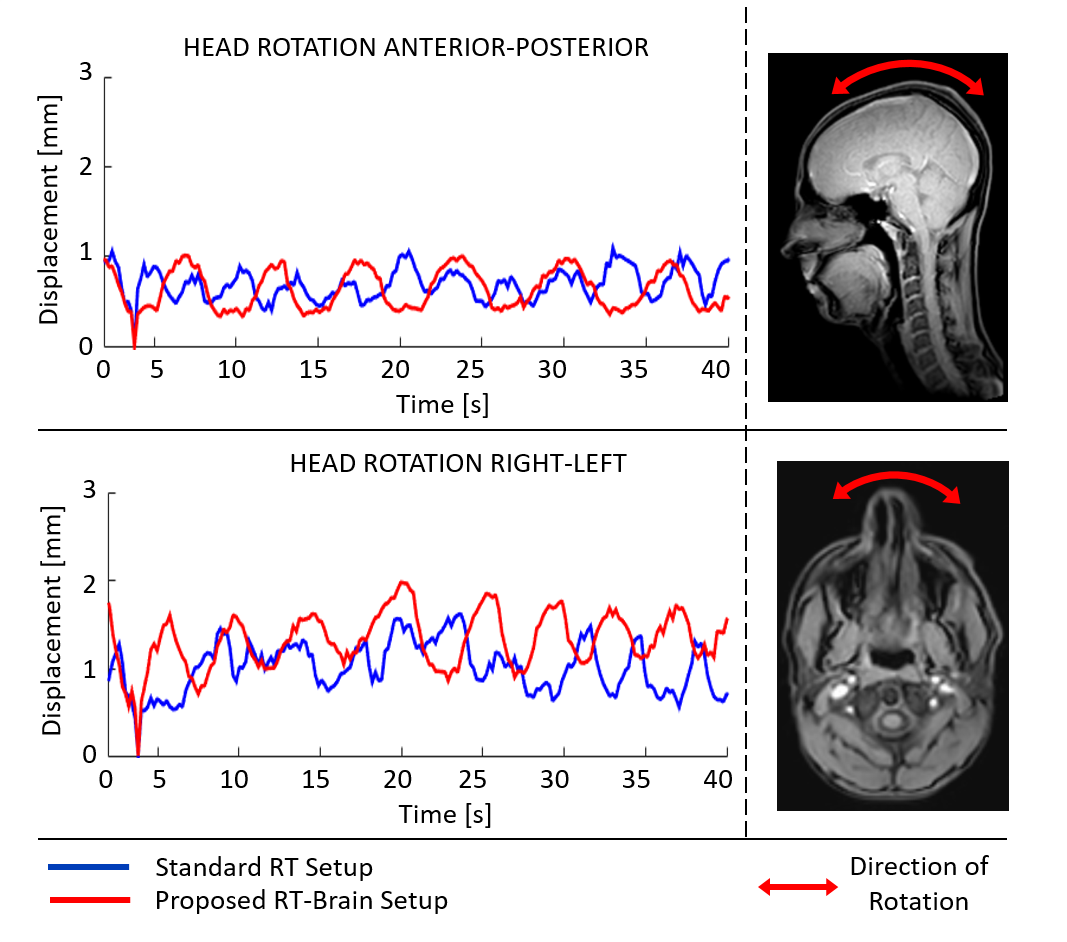
- Motion restriction test: the maximum motion in the feet-head/left-right directions was estimated from 2D cine-MR T1-weighted balanced-Fast-Field-Echo acquisitions (300 dynamics) using an Optical Flow algorithm9.
- Inter-fraction repositioning test: two high resolution 3D T1-weighted Turbo-Field-Echo sequences were acquired for each setup. Between acquisitions, the immobilization mask was removed and the subject was asked to move. The mean and standard deviation of the subject movement between each pair of MR acquisitions were computed using Optical Flow as a proxy of the reproducibility of inter-fraction subject repositioning.
Results
The proposed setup allowed between 2 and 3 times higher SNR values for brain MRI (Fig. 2-left). For the standard RT-HN setup, the SNR was highly dependent on the spatial position (Fig. 2-right). Only locally, below the flex coils, the standard RT-HN setup had comparable SNR to the proposed RT-HN setup (see transverse images). This was not the case for deeper located anatomical regions, e.g. throat, chest and shoulders (sagittal images), where the SNR of the proposed RT-HN setup was about 3 times higher.
Brain images acquired with the standard RT setup had an inferior diagnostic quality compared to the new setup, especially for the FLAIR (inferior sensitivity in detecting small lesions, Fig. 3). For HN, the image quality obtained with the standard and the proposed setups was comparable in the regions below the flex coils. However, it can be expected that the image quality is reduced for the standard HN setup in regions away from the flex coils (e.g. low neck and shoulders) due to the reduced SNR.
Comparable motion restriction in feet-head/left-right directions (maximum motion≈1mm, Fig. 4) and comparable inter-fraction repositioning accuracy (mean inter-fraction movement 1±0.5mm) were observed for the standard and the novel setup.
Discussion and Conclusions
We created an immobilization setup that fits in the diagnostic head/neck MR coils. This setup has several advantages compared to state-of-the-art setups: diagnostic image quality in RT treatment position, high SNR, homogenous signal, restricted motion (about 1 mm) and accurate inter-fraction repositioning. The presence of more receive elements in the head/neck MR coils compared to the flex coils offers more opportunity for parallel imaging. Furthermore, lack of robustness related to the use of surface flexible coils is avoided, e.g. coupling due to technician dependent coil positioning, which often results in relatively poor image quality. The translation of the new setup to the treatment table will be further investigated.Acknowledgements
The authors would like to thank Fred Groen, Tuan Nguyen, Ellart Aalbers and Teun Coolen for their assistance and support.References
1) Hess CF, et al Radiother Oncol (1995), 34:69–72.
2) Hanvey S, et al. Phys Med Biol (2009), 54:5381–94.
3) Verduijn GM, et al. Int J Radiat Oncol Biol Phys (2009), 74:630–6.
4) Ruytenberg T, et al. Front Oncol (2018), 8:216.
5) Wong OL, et al. Quant Imaging Med Surg (2017), 7:205–214.
6) Winter RM, et al. Radiother Oncol (2018), 128(3):485-491.
7) Hayes CE, et al. Med Phys (1985), 12:604–7.
8) Kellman P., et al. MRM (2005), 54:1439-47.
9) Zachiu C., et al. Phys Med Biol (2015), 60:9003–29.
Figures