1238
High-Resolution motion-corrected 2D Myocardial Perfusion MRI using Locally Low Rank and Wavelet Sparsity Constraints1Division MR Clinical Science, Philips, Best, Netherlands, 2Dept. of Biomedical Engineering, Eindhoven University of Technology, Eindhoven, Netherlands, 3Philips Health Systems, London, United Kingdom, 4School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 5Philips Healthcare, Guildford, United Kingdom, 6Philips Healthcare Iberia, Madrid, Spain, 7University of Leeds, Leeds, United Kingdom
Synopsis
First-pass perfusion cardiac MR (FPP-CMR) allows the assessment of ischemic heart disease. However, conventional FPP-CMR has limited spatial resolution and requires breath-holding. Moreover, diagnostic accuracy may be compromised due to dark-rim artifacts. Here, we propose a free-breathing quantitative high-resolution FPP-CMR framework that combines dynamically variable undersampling with a motion-corrected reconstruction approach that uses spatial and temporal constraints. The proposed motion-corrected strategy improves image sharpness and quantification of myocardial blood flow from free-breathing acquisitions. The highly undersampled acquisitions allow short acquisition windows and facilitate higher spatial resolution images, which are less sensitive to dark-rim artifacts, thus improving the diagnostic accuracy of FPP-CMR.
Introduction
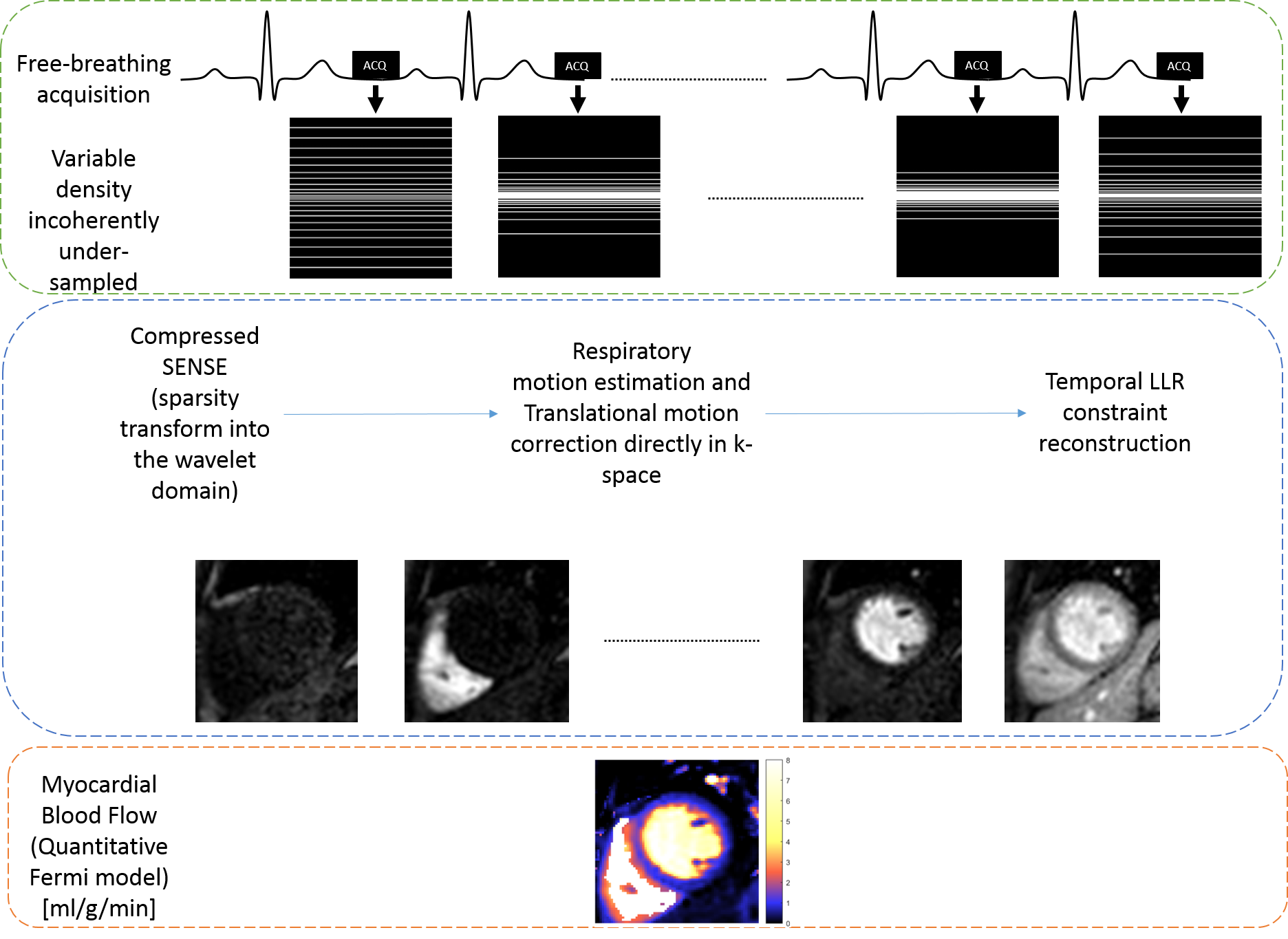
First-pass perfusion cardiac MR (FPP-CMR) provides important diagnostic and prognostic utility for noninvasive assessment of coronary artery disease (CAD)1. High-resolution FPP-CMR imaging, in comparison with conventional FFP-CMR, shows higher diagnostic accuracy and reduced dark-rim artifact2. To achieve an appropriate combination of temporal/spatial resolution and spatial coverage, fast data acquisition is required, preferably without the need for breath-holds3. Methods to accelerate4 or correct for motion5 have been proposed. In this work, we propose to combine motion correction and k-t accelerated dynamically variant undersampled Cartesian acquisitions, to achieve high-resolution FPP-CMR images. Non-rigid image registration is used to estimate respiratory motion and translational motion correction is performed directly in the k-space. Then, images are obtained using a reconstruction approach with locally low rank (LLR)6 and sparse constraints. The proposed framework was tested in 4 patients with suspected cardiovascular disease and one healthy subject.Methods
Retrospective study: Rest FPP-CMR acquisitions were performed in 4 patients using a dual-bolus technique with 0.0075 + 0.075 mmol/kg of Gadobutrol. Two patients were scanned on a 3T Philips Achieva scanner and two on a 1.5T Philips Ingenia scanner. A saturation-recovery turbo field echo (TFE) sequence was used to acquire one short-axis (SAX) slice in free-breathing. Imaging parameters were as follows: TE/TR=2.0/0.92 ms, FOV=320x320mm2, Flip Angle (FA)=15°, in-plane resolution=2.8x2.8mm2 (reconstructed to 1.67x1.67mm2), slice thickness=10mm, acquisition window=228.8ms, saturation recovery time=130ms.
Prospective study: In-vivo FPP-CMR measurements were obtained in one volunteer on a Philips Ingenia 1.5T scanner. Rest FPP-CMR was performed using a single-bolus injection of 0.05 mmol/kg. A TFE sequence was used to acquire 3 SAX slices at mid-diastole. Two different undersampling factors were used: SENSE = 2.2; CS-SENSE = 6. Acquisitions parameters: 1) Free-breathing CS-SENSE-undersampled sequences: FOV=320x320x44mm3, in-plane resolution = 1.67x1.67mm2, TR/TE = 3.0/1.42 ms, acquisition window 96.8 ms; 2) Breath-hold SENSE-undersampled sequence: FOV=360x360x44 mm3, in-plane resolution= 2.45x2.45mm2 (reconstructed to 1.4x1.4mm2), TR/TE=2.6/1.2 ms, acquisition window=110.6 ms. The following parameters were kept equal for all acquisitions: slice thickness=10 mm, FA=15°, saturation recovery time=100 ms, total scan duration=1:23 min. A variable density k-t sampling strategy was used in the undersampled acquisitions (Fig.1). The same sampling was used in the retrospective study to generate 4-fold, 6-fold and 8-fold undersampled datasets.
Reconstruction and motion correction: Firstly, the vendor's default reconstruction was used to reconstruct FPP-CMR data depending on the undersampling scheme (SENSE or Compressed-SENSE respectively). The resulting images were used to estimate the frame-by-frame translational motion by registering every frame to the sliding average of its predecessor (±7 frames). Then, motion correction was applied directly in k-space. Finally, temporal LLR and spatial wavelet (LLR+W) constraints were combined to reconstruct the motion-corrected dataset (Fig.1). Images were obtained by solving:
$$\hat{\mathbf{x}} = \arg \min\limits_{\mathbf{x}} \left\{\frac{1}{2}\left\|\mathbf{Ex}- \textbf{k}\right\|_2^2 + \alpha \sum_p \left\| \mathcal{R}_p \mathbf{x}\right\|_* + \beta \left\| \Psi\mathbf{x}\right \|_1\right\},$$ where $$$\mathbf{x}$$$ are the dynamic images, $$$\mathbf{k}$$$ is the dynamic time series data (translational motion corrected), $$$\mathbf{E}$$$ is the SENSE encoding operator, $$$\mathcal{R}_p$$$ is the operator that extracts the pth patch from $$$\mathbf{x}$$$, $$$\Psi$$$ is the spatial wavelet transform operator, $$$\alpha$$$ and $$$\beta$$$ are regularization parameters. For a given vector $$$u$$$, $$$\left\| u\right\|_* $$$ represents the nuclear norm of $$$u$$$ (sum of singular values) and $$$\left\| u\right\|_1 $$$ is the L1-norm of $$$u$$$. The problem was solved using the Alternating Direction Method of Multipliers.
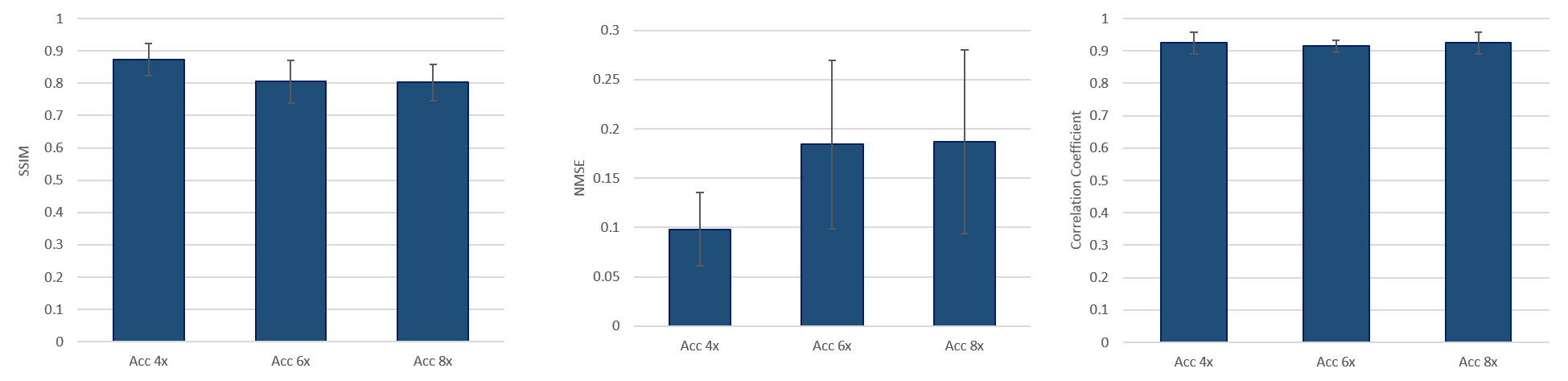
Retrospectively undersampled 2D Cartesian reconstructions were quantitatively evaluated against fully-sampled data using normalized mean square error (NMSE), structural similarity (SSIM) index and correlation coefficient. Quantitative myocardial blood flow (MBF) was calculated using the Fermi model-based deconvolution7.
Results
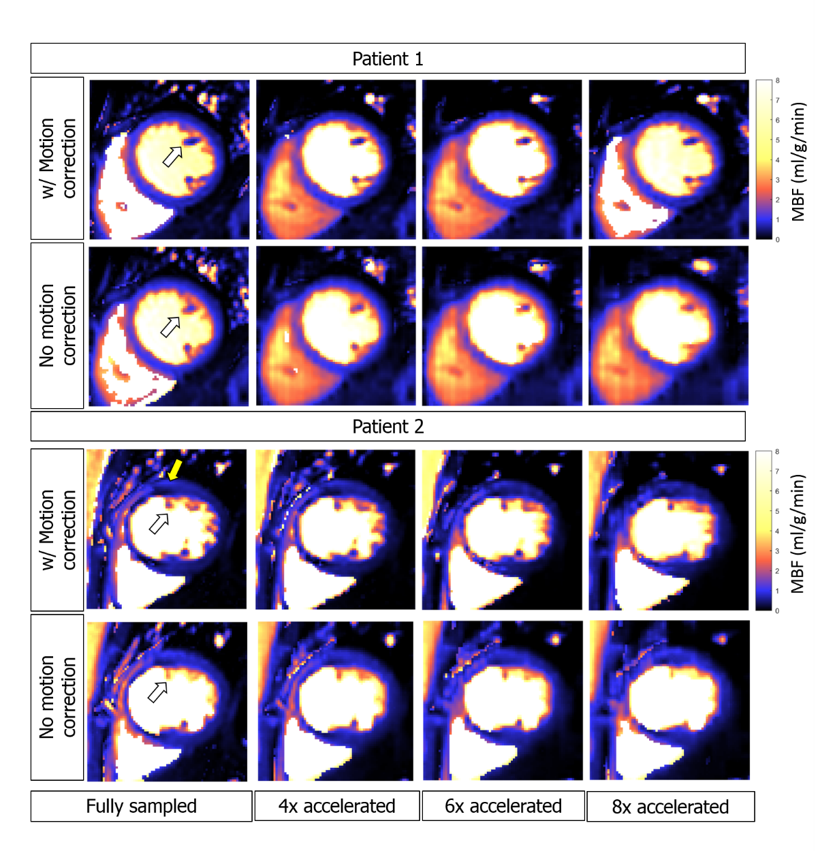
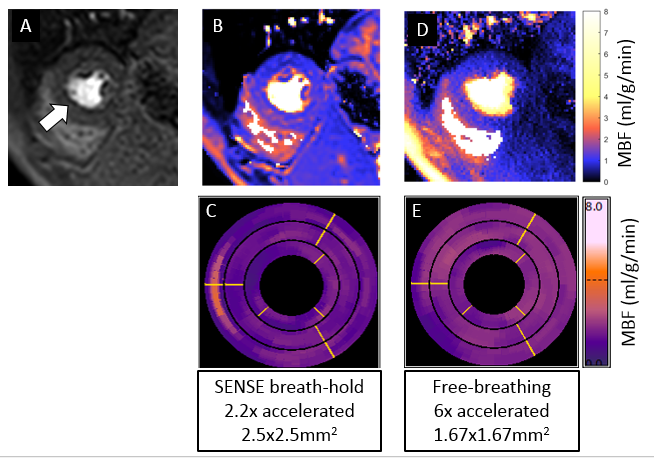
Figure 2 shows the images obtained for two representative patients for the retrospective study, showing the effect of motion correction and acceleration. The MBF maps obtained for two subjects are displayed in Figure 3. Figure 4A shows a small decrease of SSIM with higher acceleration factors but remains high (on the order of 0.8). Similarly, Figure 4B shows that NMSE is increased for the higher accelerations, but remains relatively small at around 0.2. Figure 4C confirms the excellent agreement between the fully sampled and the retrospectively undersampled datasets, for all motion-corrected accelerated datasets (R2>0.9). Figure 5 shows the quantitative MBF maps for the prospective study. The high-resolution images obtained with the proposed LLR+W reconstruction ameliorate the dark-rim artifact (Fig 5A) present in the standard-resolution scan. Conversely, the maps and bullseye plots demonstrate improved homogeneity of LLR+W over the standard protocol, which also suffered from residual motion in the basal slice.Conclusion
High-resolution accelerated FPP-CMR is enabled by combining 2D variable undersampling, LLR+W reconstruction and motion correction. The proposed strategy greatly reduces motion artifacts and improves image quality allowing for higher resolution, thus minimizing dark-rim artifacts and improving MBF quantification in free-breathing FPP-CMR.Acknowledgements
This work was supported by: MRC Proximity to Discovery: Industry Engagement Fund, Wellcome EPSRC Centre for Medical Engineering (NS/A000049/1). This work was supported by the European Commission within the Horizon 2020 Framework through the MSCA-ITN-ETN European Training Networks (project number 642458).
References
- Nagel E, Klein C, Paetsch I, Hettwer S, Schnackenburg B, Wegscheider K, Fleck E. 2003. Magnetic resonance perfusion measurements for the noninvasive detection of coronary artery disease. Circulation. 108(4):432-437.
- Motwani M, Maredia N, Fairbairn TA et al. High-resolution versus standard resolution cardiovascular MR myocardial perfusion imaging for the detection of coronary artery disease. Circ. Cardiovasc. Imaging 5, 306–313 (2012).
- Chen X, Salerno M, Yang Y, Epstein FH. Motion-compensated compressed sensing for dynamic contrast-enhanced MRI using regional spatiotemporal sparsity and region tracking: block low-rank sparsity with motion-guidance (BLOSM). Magn Reson Med. 2014;72(4):1028-38. .
- Otazo R, Kim D, Axel L, Sodickson DK. Combination of compressed sensing and parallel imaging for highly accelerated first-pass cardiac perfusion MRI. Magn Reson Med 2010;64:767–776.
- Kellman P, Hansen MS, Nielles-Vallespin S, Nickander J, Themudo R, Ugander M, et al. Myocardial perfusion cardiovascular magnetic resonance: optimized dual sequence and reconstruction for quantification. J Cardiovasc Magn Reson. 2017;19:43.
- Zhang, C., Nakarmi, U., Li, H., Zhou, Y., Liang, D., & Ying, L. (2018). Accelerating T2 Mapping Using a Self-trained Kernel PCA Model, 5–6.
- Jerosch-Herold M, Wilke N, Stillman AE. Magnetic resonance quantification of the myocardial perfusion reserve with a Fermi function model for constrained deconvolution. Med Phys. 1998;25(1):73-84.
Figures